

AI-predicted dose is not a single product category. In radiotherapy, the same wording may refer to a 3D dose distribution used as a starting point for planning objectives, a deep learning model that generates a reference dose for dose mimicking, or an optimization automation layer that does not replace physical dose calculation.
That distinction matters when comparing MVision Dose+, RayStation deep learning planning, and OptiPlan. All three sit inside the broader move toward automated planning, but they do not have the same technical role.
Short answer
- MVision Dose+ is presented as dose-prediction software that generates clinically achievable VMAT dose distributions from CT images and structures, importable into a TPS through DICOM.
- RayStation uses deep learning models to predict a dose image that can serve as a reference for mimic optimization inside the TPS.
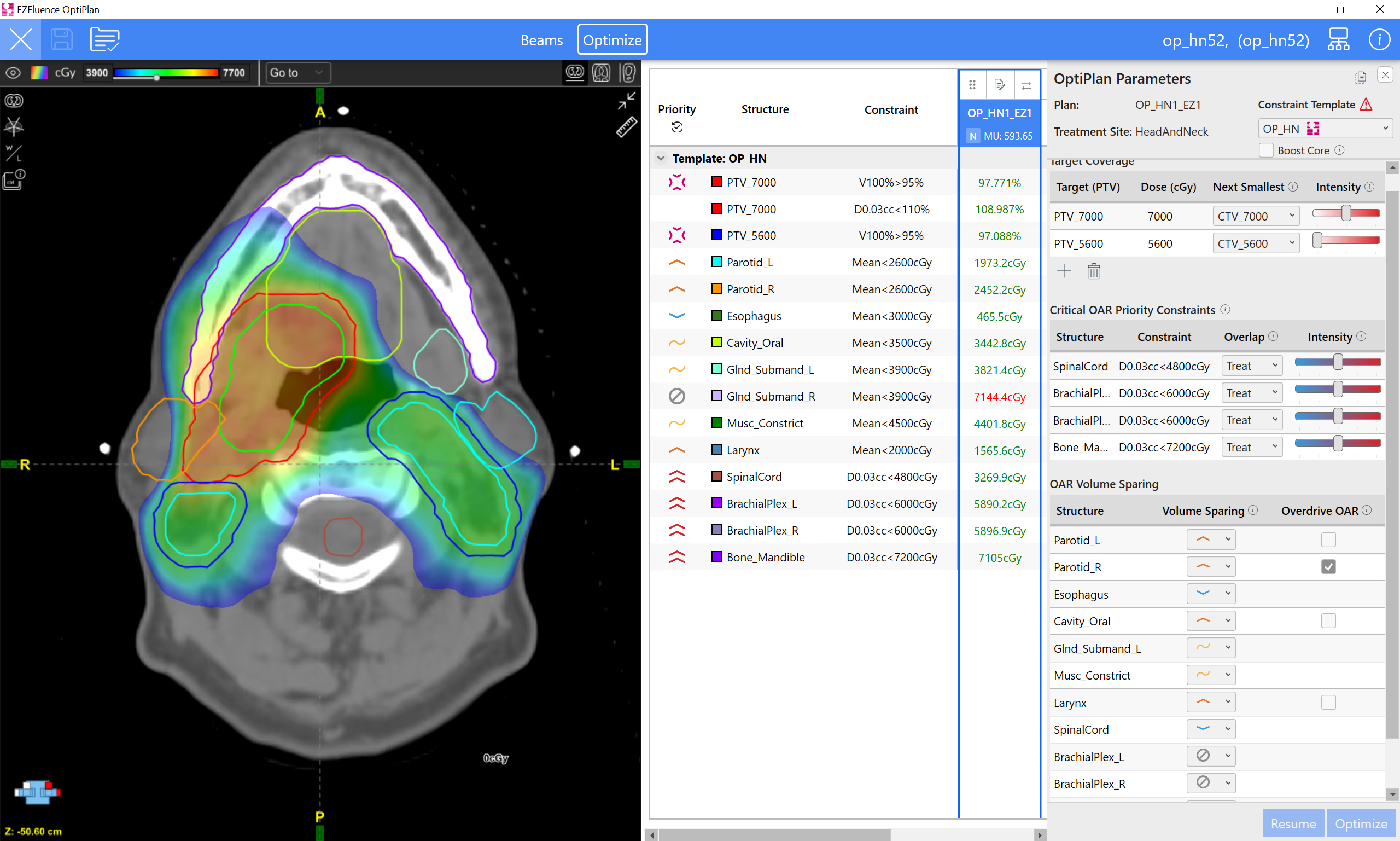
- OptiPlan should be described as VMAT planning automation using TPS-native optimization tools and ClearCheck objectives. Current public material does not describe it as an AI dose engine.
Dose prediction is not particle transport
An algorithm such as Monte Carlo simulates physical transport and energy deposition. A predicted-dose model learns a relationship between anatomy, structures, prescription, beam setup or approved examples and a likely dose distribution. That output may reduce trial-and-error, but it remains constrained by the training domain and local validation.
Clinically, the value is not that a neural network replaces the TPS. The value is that it can anticipate a plausible dose, expose whether a case is straightforward or constrained, and guide objectives before repeated manual iterations.
Technical comparison
| System | Publicly described role | Likely clinical use | Editorial caution |
|---|---|---|---|
| MVision Dose+ | Personalized VMAT dose prediction from CT and structures | Initial dose and objective setting before TPS refinement | Validate by site, protocol, TPS, fractionation, and patient population |
| RayStation deep learning planning | Voxel-level prediction with U-net based models and dose mimicking | Executable plan generated inside RayStation and refined as a conventional plan | Separate predicted dose from final calculation and clinical approval |
| Radformation OptiPlan | VMAT optimization automation with TPS tools and ClearCheck | Reduced iteration and lower planner variability | Do not call it AI dose prediction without specific documentation |
MVision Dose+: 3D distribution as a starting point
The Dose+ page states that the product creates achievable VMAT distributions from CT images and structure sets using a simple DICOM transfer. The important technical point is that the model produces a 3D dose distribution that can enter the planning workflow.

The NCCC Newcastle case study is useful because it compares Dose+ against automated and manual workflows in prostate cases. The relevant lesson is not a single metric, but the way a department can validate a prediction tool inside a specific TPS and clinical protocol.

RayStation: predicted dose for mimic optimization
RaySearch describes a model that receives a multichannel structure volume and outputs a voxel-level dose image. The predicted dose is stored in RayStation and can be used as a reference for mimic optimization. The final plan remains inside the TPS and can be refined and evaluated conventionally.

This connects to the existing article on RayStation collapsed cone and Monte Carlo: deep learning can generate a planning reference, while the physical dose engine calculates the final plan.
OptiPlan: VMAT automation, not an AI dose engine
Radformation positions OptiPlan as VMAT planning automation that uses TPS-native tools and ClearCheck-driven objectives. As of June 15, 2026, public OptiPlan material described it as a feature of the newest EZFluence version with FDA 510(k) pending.
The accurate comparison is therefore operational: OptiPlan addresses manual iteration and planning variability, while MVision Dose+ and RayStation deep learning planning are closer to the specific idea of predicting a dose distribution to guide planning.
Where the medical physicist remains central
- Define the intended use: triage, reference dose, optimization objective, pre-planning, or review support.
- Separate predicted dose, optimized plan, and approved final calculation.
- Connect adoption to commissioning and QA.
- Use clinical and worst-case metrics, not only average gamma. The detailed checklist is in how to validate AI-predicted dose.
FAQ
Does AI-predicted dose replace Monte Carlo?
Not as a general rule. It can accelerate planning decisions, but clinical equivalence must be demonstrated for the intended use. Physical dose calculation, independent checks, and local validation remain safety barriers.
Do MVision Dose+ and RayStation do the same thing?
Both use dose prediction, but the integration is different. Dose+ is presented as software that exports a DICOM dose distribution to the TPS; RayStation integrates the predicted dose into its planning environment for mimic optimization.
Is OptiPlan AI dose prediction?
Based on the public material reviewed, that is not the right description. It is better described as VMAT automation driven by objectives and TPS optimization tools.
References
- MVision AI Dose+. https://mvision.ai/dose/
- NCCC Newcastle Dose+ case study. https://mvision.ai/case-study-evaluating-ai-dose-prediction-across-standard-and-complex-prostate-cases-at-nccc-newcastle/
- RaySearch: Machine Learning in RayStation. https://www.raysearchlabs.com/machine-learning-in-raystation/
- RaySearch white paper: Deep learning planning. https://www.raysearchlabs.com/media/publications/white-papers/deep-learning-planning/
- Radformation OptiPlan. https://radformation.com/optiplan/optiplan
- Radformation webinar: Introducing OptiPlan. https://resources.radformation.com/webinar-introducing-optiplan-automated-vmat-planning


