

The integration of MRI with linear accelerators represents one of the most significant developments in image-guided radiotherapy of the last decade. Systems such as the Elekta Unity (1.5 T) and ViewRay MRIdian (0.35 T) allow you to visualize tumors and critical structures with soft tissue resolution in real time during irradiation. This capability opens up concrete perspectives for daily plan adaptation (online adaptive radiotherapy) and for reducing planning margins in high mobility sites such as the lung, prostate and pancreas.
However, the presence of the static magnetic field introduces physical disturbances that algorithms configured for field-free environments do not represent. The field modifies the trajectories of secondary electrons, alters the dose distribution at the interfaces and can produce clinically relevant differences in geometries with air and low density. The correct conclusion is not that an algorithmic family is always invalid, but that the engine used in MR-Linac needs to explicitly incorporate the field and be validated for the specific business setting.
This article discusses the physical mechanisms underlying these effects, how treatment planning systems (TPS) computationally model them, the commissioning and quality control (QA) requirements specific to MR-Linac, and the practical implications for the anatomical sites most frequently treated on this platform. The distinctions between established physical description, commercial implementation and evidence of clinical validation are made clear throughout the text.
In this Article
- 1. Why Adding a Magnetic Field Changes Dosimetry
- 2. Lorentz force and electron return effect
- 3. Electron streaming in cavities and regions outside the field
- 4. How Monte Carlo and GPUMCD model the problem
- 5. Electron density, synthetic CT and material assignment
- 6. MR-Linac Specific Commissioning and QA
- 7. Implications for lung, esophagus, breast and pelvis
- 8. FAQ
- 9. References
Why Adding a Magnetic Field Changes Dosimetry
In conventional accelerators, dose deposition by a photon beam is mediated primarily by secondary electrons. Clinical implementations designed only for zero magnetic field do not include the Lorentz force in electronic transport. Therefore, the generic name of the algorithm is not enough: it is necessary to confirm whether the version of TPS was developed and commissioned for the magnetic geometry of the equipment.
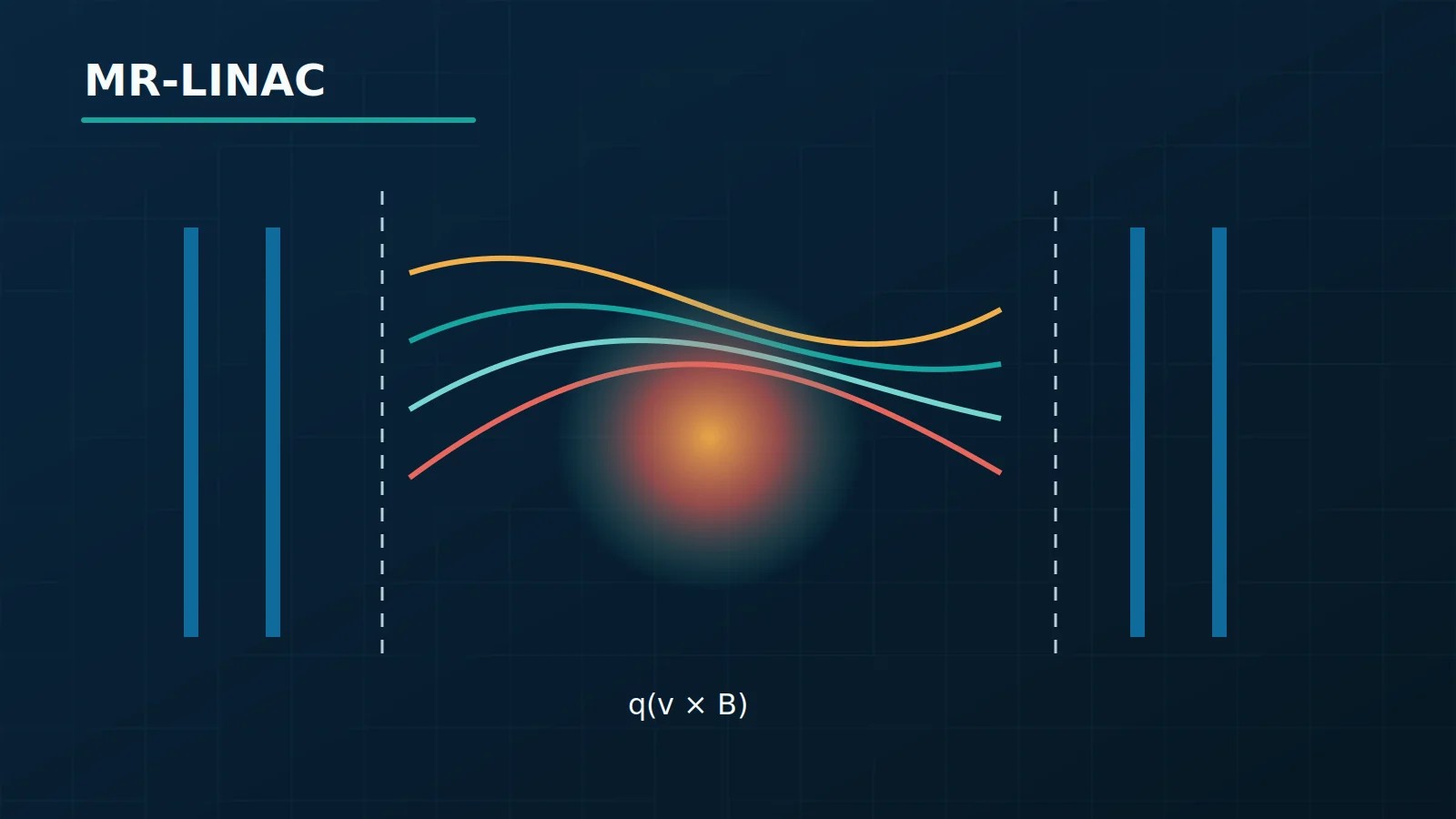
When a static magnetic field B is superimposed on the irradiated volume, the force F = q(v × B) deflects each charged electron from its linear path. For electrons of typical energy in photon therapy (2–20 MeV), the radius of curvature in Unity’s 1.5 T field is on the order of centimeters — comparable to the proper range of these electrons in soft tissue. The result is that the dose distribution is no longer axially symmetrical and begins to depend on the orientation between the Bfield, the photon beam and the material interfaces present in the patient’s geometry. Photons, being neutral, are not deflected; only secondary electronic transport is disturbed.
Three practical consequences emerge directly from this fact. First, even in a homogeneous field, the deflection of electrons in the plane perpendicular to B creates asymmetry in the beam profiles, observable in measurements with ionization chambers or films. Second, at boundaries between tissue and air (chest wall over lung, esophageal mucosa, skin surface), the abrupt change in electron density amplifies the deviation, producing localized over- or underdosage depending on geometry and orientation. Third, the so-called electron return effect (ERE) emerges, described in the following section, which is physically distinct from mere profile asymmetry.
The review of Sim et al. (2020) systematizes the physical challenges in MR-guided radiotherapy, covering dose perturbation, instrumentation and QA. It explicitly distinguishes between what is physically well established, what has been validated in clinical conditions, and what remains under investigation — a distinction that should guide implementation in any service.
Lorentz force and electron return effect
ERE is the most widely documented phenomenon of the interaction between magnetic field and dosimetry in MR-Linac. It occurs when secondary electrons penetrate regions of low electron density (lung, intraluminal air) and, instead of dispersing progressively as they would without a field, they describe curved trajectories that return them to the adjacent high-density tissue. The result is a dose spike at the surface of the “recipient” tissue—for example, in the inner wall of a tumor adjacent to the lung, or in the esophageal mucosa adjacent to air.
The most common configuration in Unity is a beam perpendicular to B (field parallel to the cranio-caudal axis, beam entering laterally). In this configuration, the ERE is more pronounced because the electrons emitted forward from the interaction point have a velocity component in the plane where the Lorentz force is maximum. For a beam parallel to B, electrons tend to spiral along the field lines, reducing the ERE but favoring electron streaming (next section).
The magnitude of the ERE depends on four main variables: magnetic field intensity (larger field → greater curvature → more pronounced ERE), beam energy (higher energy beams produce electrons with greater radius and, therefore, greater return distance), angle between beam and field, and interface geometry (flat, concave or convex). These dependencies were characterized in bench work, with ionization chambers and films, in reference geometries with solid and water phantoms.
It is essential to distinguish the evidence available in different contexts. ERE as a physical phenomenon in simple geometries is well established and is reproduced by validated Monte Carlo simulations. Quantitative extrapolation to complex clinical geometries — with irregular tumor, multiple interfaces, and intrafraction variation — is the subject of active research and has uncertainties that need to be considered in clinical planning.
Electron streaming in cavities and regions outside the field
When the beam is parallel to the magnetic field, secondary electrons tend to follow the field lines instead of scattering laterally. This phenomenon, called electron streaming, produces narrow and highly localized beams of electrons that cross cavities (trachea, esophagus, intestine) and regions peripheral to the treatment field with significantly greater fluence than would be expected in the absence of a field.
electron streaming has two distinct practical consequences. The first is the increase in peripheral dose — relevant for organs at risk far from the target, particularly in pediatric patients or when radiosensitive structures are close to the field. The second is dose deposit in filamentary patterns within air or intestinal gas cavities, a pattern that fieldless deterministic algorithms do not model. The experimental detection of electron streaming requires dosimeters with high spatial resolution — radiochromic films or 2D arrays of small detectors — as the phenomenon manifests itself in narrow regions.
The most important practical implication is that MR-Linac QA protocols must include out-of-field dose verification as an explicit component. In conventional accelerators, the peripheral dose outside the field is small and rarely checked directly. In MR-Linac, electron streaming can produce peripheral doses not predicted by conventional algorithms. This point is a real failure scenario, not a hypothetical one, and should be included in the training of the medical physics team.
How Monte Carlo and GPUMCD model the problem
The natural solution for particle transport in a magnetic field is the Monte Carlo (MC) method. Simulators such as EGSnrc, GATE/Geant4 and MCNP allow including the Lorentz force explicitly in the electronic transport step, adding the term qv × B to the equation of motion at each step. Validated MC codes reproduce ERE, electron streaming , and profile asymmetries with adequate fidelity from experimental data in reference geometries, making them the benchmark for validating commercial algorithms.
The clinical challenge is calculation time. Reducing statistical uncertainty increases the number of particle histories and computational cost, while online adaptation imposes a short operational window. Performance must be measured on the hardware, grid, and uncertainty protocol used by the service itself.
GPUMCD originally emerged as a GPU-oriented Monte Carlo platform, not as an algorithm created specifically for Unity. Later commercial implementations may incorporate the magnetic field and integrate Monaco/Unity streams, but this capability is product and version dependent. The same goes for the dose magnitude: you should not assume dose to medium or dose to water without consulting the documentation and data exported by the commissioned version.
Table 1 — Comparison of dose calculation algorithms in the context of MR-Linac
| Family | Type | Requirement for MR-Linac | Limitation if used without field adaptation |
|---|---|---|---|
| Pencil Beam / kernel | Analytical or semi-analytical | Model explicitly validated with field B | May lose asymmetry, ERE and streaming |
| LBTE solver | Deterministic | Transport term compatible with magnetic geometry | The name LBTE alone does not guarantee support for the field |
| Monte Carlo on GPU | Stochastic | Electronic transport with Lorentz force and local beam model | Result depends on materials, grid, statistics and independent beam model |
| Monte Carlo | Stochastic | Validated code and geometry for the field studied | Cost and integration may limit online use |
GPUMCD is a commercial implementation whose clinical validations continue to accumulate evidence. Validations on reference geometries are more robust than validations on complex clinical cases. Scenarios that may challenge the model’s assumptions include bulky metallic implants close to the target, anatomies with air cavities of extremely irregular geometry, and patients outside the range of variation covered by local commissioning.
Electron density, synthetic CT and material assignment
In conventional planning, simulation CT provides Hounsfield numbers (HU), converted into relative electron density via the HU-ρe calibration table. In MR-Linac, the image available in real time is an MRI, whose signal has no direct physical relationship with the electron density. Three approaches are used to work around this problem:
Bulk density assignment: contoured structures receive fixed electron density values from reference tables (soft tissue, bone, lung, air). It is the fastest method and the most used clinically, but it introduces errors when the real anatomy deviates from the reference — hyperinflated versus atelectatic lungs, for example, can have densities that are very different from the assigned reference value.
Synthetic CT (sCT): machine learning algorithms or atlas bases generate a pseudo-CT image from the MRI, with HU values approximated pixel by pixel. It allows dose calculation with complete spatial resolution and captures local heterogeneities not covered by bulk density. Fails when the MRI has motion artifacts, strong magnetic susceptibility (near prostheses), or when the patient’s anatomy is outside the model’s training distribution.
Reference CT with deformable registration: the initial planning CT is deformably registered to the MRI of the day. Useful for early fractions, but accumulates uncertainty as anatomy changes — new pleural effusion, rectal filling variation, or significant weight loss may invalidate the recording.
Each approach has implicit hypotheses and failure scenarios that must be documented in the service’s clinical protocol. Validation of the chosen method must be an explicit part of the commissioning process, with tests on phantoms with known densities. The protocols published by Cusumano et al. (2022) describe this type of evaluation as a requirement before clinical use.
MR-Linac Specific Commissioning and QA
Commissioning an MR-Linac has all the complexities of a conventional accelerator plus challenges specific to the magnetic field environment. The protocol described by Winkel et al. (2019) for Unity it covers everything from output measurements and beam profiles to absolute dose verification in phantoms with an active magnetic field, and is a starting point for the development of local protocols.
Key instrumental challenges include ionization chambers — whose response factor is affected by the magnetic field in a manner dependent on the orientation of the chamber relative to B — and detector arrays, which must be field-specifically qualified before clinical use. Radiochromic films (EBT3, EBT-XD) are the most robust dosimeters for 2D distribution verification, as they are not directly affected by the magnetic field. MOSFET and TLD dosimeters require individual validation in the field environment prior to any clinical use.
Table 2 — MR-Linac specific QA components and their particularities
| QA component | MR-Linac specific challenge | Note |
|---|---|---|
| Absolute output (cGy/UM) | Chamber correction factor in field B (orientation dependent) | Check with kB factor determined in commissioning |
| Beam profiles | B-induced asymmetry; check vs. baseline data | Active B field during measurement |
| RT/MRI isocenter coincidence | Mechanical isocenter must coincide with image isocenter | Dedicated tool (adapted Winston-Lutz phantom) |
| Out-of-field dose | Electron streaming without equivalent in conventional linac | High spatial resolution dosimeters required |
| Material assignment (sCT/bulk) | Validation in phantom with known densities | Repeat after TPS software updates |
| Individual plan verification | Dose in phantom with active B field | Format (2D, 3D, point) defined in local protocol |
| MRI image geometry | Gradient distortion affects target location | Geometric distortion phantom; monthly frequency |
| QA of the adaptive process | Registration + recontouring + re-optimization: each step with source of error | Periodic audit of the complete chain |
An often underestimated aspect is the QA of the online adaptation process as an integrated chain. Checking only isolated components (output, profiles, geometry) does not guarantee that the final product — the adapted plan delivered to the patient — is correct. The adaptation chain involves image registration, automatic recontouring, plan re-optimization and dose recalculation; any step may introduce error not captured by individual checks.
Implications for lung, esophagus, breast and pelvis
The clinical relevance of the dosimetric effects of the magnetic field is heterogeneous between anatomical sites, being proportional to the presence and variability of air-tissue interfaces.
The lung is a particularly sensitive site. The low density of the parenchyma increases the relevance of interfaces and the lack of electronic balance. Accuracy requires a motor that models the magnetic field and has been validated in this geometry; applying an implementation intended for null field is not an acceptable replacement.
Esophagus presents the additional challenge that intraluminal air volume varies between fractions—swallowing, reflux, positioning. The ERE in the air-adjacent esophageal wall creates local dose peaks, but the exact position of these peaks changes with the geometry of the cavity. Online adaptation allows monitoring this variability, which would be invisible to conventional IGRT systems; however, the dose to the mucosa is difficult to predict accurately if the contour of the air cavity is not updated with each fraction.
Breast includes tissue-air interfaces at the skin surface where ERE can result in elevated surface dose in certain field and gantry orientations. In hypofraction regimens, where the dose per fraction is higher and tolerance to the cutaneous dose is a limiting factor, this effect has direct clinical implications. Surface dosimetry on MR-Linac requires specific dosimeters (extrabolus films, thin surface detectors) that must be part of the commissioning protocol.
Pelvis (prostate, cervix, rectum) has a smaller proportion of air than the lungs and esophagus, which reduces the magnitude of the ERE in relation to these sites. However, interfaces with the rectum and bladder remain relevant, especially when there is variable rectal gas between fractions. The main clinical benefit of MR-Linac in the pelvis is the superior visibility of soft tissue on MRI, which allows accurate delineation of prostate, seminal vesicles and lymph node structures without contrast. The dosimetric validation evidence is more robust for the pelvis than for the lung and esophagus, which reflects both the number of centers treating prostate in MR-Linac and the lower dosimetric complexity of the site.
Application of MR-Linac to less studied sites — such as pancreas, liver, and head and neck tumors — requires additional caution and ideally prospective collection of dosimetric data as part of formal research protocols.
FAQ
Can GPUMCD be used for all Unity clinical cases without restrictions?
The Monte Carlo implementation provided for the clinical equipment flow includes magnetic field modeling, but its limits remain defined by product, version and commissioning. Implants, complex cavities, and anatomies outside the test set may warrant additional verification. The local protocol must record these limits without assuming that the GPUMCD name guarantees identical behavior on all platforms.
What is the practical difference between dose to medium (D~m~) and dose to water (D~w~) in the context of MR-Linac?
The reported convention must be confirmed in the clinical version. D~m~ and D~w~ are not interchangeable labels, especially in materials whose composition differs from water. The practical problem arises when historical constraints and the calculated distribution use different conventions; this relationship must be documented in the implementation process.
Is synthetic CT generated from MRI accurate enough to replace planning CT at all sites?
Not universally. The accuracy of sCT varies by anatomical site, image quality and generation method (machine learning, atlas or bulk density). For pelvis, published results are generally favorable. For lung, the variability of parenchymal density and the greater sensitivity to ERE make the accuracy of sCT more critical. Validation of the chosen method must be carried out locally, with phantoms of known density, and not just assumed from publications from other centers with potentially different hardware and software.
Which dosimeters are suitable for dose verification in a magnetic field?
Radiochromic films (EBT3, EBT-XD) are the most robust option for 2D distributions as they are not directly affected by the static magnetic field. Ionization chambers can be used for spot dose with correction factors specific to the orientation of the chamber relative to B — these factors must be determined at commissioning, not assumed from publications with different geometries. MOSFET and TLD dosimeters require individual field validation prior to clinical use. Detector arrays must be specifically qualified; Not all commercial models are suitable without modifications or correction factors documented by the manufacturer.
Does MR-Linac eliminate the need for conventional image QA?
No. MR-Linac adds QA requirements related to the magnetic field and online adaptation chain, but does not eliminate image QA requirements. The geometric distortion of MRI by gradients and magnetic susceptibility is a relevant source of error: if the tumor appears in a position displaced by gradient distortion, the treatment will be poorly centered regardless of the quality of the dose calculation. MRI image geometry QA — distortion, resolution, contrast — is a mandatory component of the QA program. Furthermore, the QA of the adaptive process as an integrated chain (registration + recontouring + re-optimization + recalculation) must be audited periodically, as errors can arise in the integration of steps even when each individual component is within specification.
References
-
Yes AJ, Korreman SS, Vestergaard A. Physical challenges in magnetic resonance image-guided radiotherapy. Acta Oncol. 2020. https://pubmed.ncbi.nlm.nih.gov/32370788/
-
Winkel D, Bol GH, Kroon PS, van Asselen B, Hackett SS, Werensteijn-Honingh AM, et al. Adaptive radiotherapy: the Elekta Unity MR-linac concept clinical implementation in an MR-linac consortium. Radiother Oncol. 2019. https://pubmed.ncbi.nlm.nih.gov/32432405/
-
Cusumano D, Boldrini L, Dhont J, Fiorino C, Green O, Grimwood A, et al. Artificial intelligence in magnetic resonance guided radiotherapy: Medical and physical considerations on state of art and future perspectives. Phys Med. 2022. https://pubmed.ncbi.nlm.nih.gov/35235188/
-
Raaijmakers AJE, Raaymakers BW, Lagendijk JJW. Integrating an MRI scanner with a 6 MV radiotherapy accelerator: dose increase at tissue-air interfaces in a lateral magnetic field due to returning electrons. Phys Med Biol. 2005;50(7):1363–1376.
-
Raaijmakers AJE, Raaymakers BW, van der Meer S, Lagendijk JJW. Integrating an MRI scanner with a 6 MV radiotherapy accelerator: impact of the surface orientation on the entrance and exit dose due to the transverse magnetic field. Phys Med Biol. 2007;52(4):929–939.
-
Kirkby C, Stanescu T, Rathee S, Carlone M, Murray B, Fallone BG. Patient dosimetry for hybrid MRI-radiotherapy systems. Med Phys. 2008;35(3):1019–1027.
-
Keyvanloo A, Burke B, Warkentin B, Tadic T, Rathee S, Kirkby C, et al. Skin dose in longitudinal and transverse MRI-linac systems using Monte Carlo and realistic 3D MRI field models. Med Phys. 2012;39(10):6509–6521.
-
O’Brien DJ, Roberts DA, Ibbott GS, Sawakuchi GO. Reference dosimetry in magnetic fields: formalism and measurements. Med Phys. 2016;43(8):4915–4927.


