Nasopharyngeal carcinoma target delineation demands a level of anatomical precision that few other head and neck subsites require. The nasopharynx sits deep within the skull base, surrounded by critical neural and vascular structures, and the disease has a well-documented propensity for submucosal spread, perineural invasion along cranial nerve pathways, and early bilateral nodal involvement. Unlike oral cavity or laryngeal primaries where surgical margins guide adjuvant volumes, nasopharyngeal carcinoma (NPC) is treated definitively with radiation — making the accuracy of every contoured structure the single most consequential decision in the treatment chain. This article provides a comprehensive, slice-by-slice approach to GTV, CTV, and PTV definition for NPC based on current consensus guidelines, with particular attention to skull base anatomy, nodal coverage, and dose prescription schemes used in contemporary IMRT protocols. For broader context on contouring methodology across all sites, refer to our complete guide to target volume delineation.
- Pre-Treatment Workup and Imaging Requirements
- Simulation Setup and CT Acquisition
- GTV and CTV70: Contouring Gross Disease
- CTV54-59.4: High-Risk Subclinical Volume
- Nodal Target Volumes: Bilateral Coverage Strategy
- Dose Prescription Tables and PTV Margins
- Skull Base Anatomy: Foramina, Clivus, and Cavernous Sinus
- Advanced and Recurrent Disease: T4 Considerations
- Adaptive Replanning and MRI-Guided Response Assessment
- Key References
Pre-Treatment Workup and Imaging Requirements
Accurate delineation begins well before the patient enters the CT simulator. A thorough physical examination including flexible nasopharyngoscopy is non-negotiable. The endoscopic assessment must systematically evaluate the anterior nasal space, the nasopharyngeal vault and lateral recesses (fossae of Rosenmüller), the posterior choana, and the oropharynx. Any mucosal abnormality, submucosal bulging, or cranial nerve deficit noted on exam directly influences target definition.

Diagnostic contrast-enhanced MRI is the cornerstone imaging study and must be fused to the planning CT. MRI should ideally be acquired in the treatment position, though this is not always feasible. T1-weighted non-contrast sequences are indispensable for detecting marrow infiltration at the skull base and clivus — a finding that CT routinely misses. T2-weighted and post-gadolinium T1 sequences delineate soft-tissue extent through the parapharyngeal space, retrostyloid compartment, and intracranial extension with far greater sensitivity than CT alone. MRI is absolutely critical for any patient with suspected skull base erosion, perineural disease along V2 or V3, or cavernous sinus involvement.
PET/CT plays a supplementary role. For the primary tumor, FDG uptake may both underestimate (missing submucosal or perineural spread) and overestimate (inflammatory uptake in adjacent mucosa) the true disease extent. However, PET/CT is extremely valuable for identifying small nodal metastases, particularly retropharyngeal nodes that may be borderline on size criteria alone. EBER status should be confirmed from biopsy specimens, and plasma EBV DNA titers obtained when available — both carry prognostic significance and may influence treatment intensity decisions in the context of protocols such as NRG HN001.
Simulation Setup and CT Acquisition

Patients are simulated supine with the head and neck in a neutral position. A 5-point thermoplastic mask provides immobilization from vertex to shoulders. The planning CT is acquired at 2–3 mm slice thickness with intravenous contrast, covering from the vertex to at least 2 cm below the sternoclavicular joints. This inferior extent ensures adequate coverage of level IV and supraclavicular nodes. If MRI fusion is planned — and it should be — acquiring the diagnostic MRI in the same immobilization device and head position substantially improves registration accuracy, particularly at the skull base where even 2–3 mm of rotational misregistration can shift critical contour boundaries.
One practical point that deserves emphasis: always review the planning CT in bone windows. The foramina ovale, rotundum, and lacerum are visible on bone algorithm reconstructions, and their integrity (or erosion) directly determines whether the cavernous sinus and Meckel’s cave must be included in the high-dose or intermediate-dose volume. This step is frequently overlooked, yet it changes the CTV in a meaningful percentage of cases.
GTV and CTV70: Contouring Gross Disease
The GTV encompasses all gross disease identified on physical examination and imaging. For the primary tumor, this includes the visible nasopharyngeal mass, any skull base invasion demonstrated on MRI (particularly marrow replacement on T1-weighted images), and perineural spread along cranial nerve pathways. For nodal disease, GTV includes all lymph nodes meeting size criteria (short axis ≥1 cm), any node with central necrosis regardless of size, and any FDG-avid node on PET/CT. When doubt exists about whether a node is pathologic, it should be contoured as GTV — the consequences of geographic miss in the neck are far more devastating than a modest increase in treated volume.
CTV70 is generated by expanding the GTV by 3–5 mm to account for microscopic extension beyond the visible tumor boundary. In regions where the treating physician is confident that the GTV boundary accurately represents the true disease extent — for instance, where tumor abuts an intact bony cortex — the CTV may equal the GTV with 0 mm expansion. Near critical structures, particularly the optic apparatus, the philosophy differs depending on laterality: when tumor approaches the ipsilateral optic nerve, coverage is maintained even at the cost of ipsilateral visual compromise, while constraining the contralateral optic nerve and chiasm strictly. For nodal CTV70, the same 3–5 mm expansion principle applies around grossly involved nodes. Small but clearly pathologic nodes may be prescribed an intermediate dose of 63–66 Gy. The contouring approach for NPC nodal volumes shares principles with techniques used in oropharyngeal carcinoma delineation, though the retropharyngeal compartment receives far greater emphasis in NPC.
CTV54-59.4: High-Risk Subclinical Volume for the Primary
The intermediate-dose CTV for NPC is arguably the most complex subclinical volume in all of radiation oncology. It must account for the multiple routes of spread from the nasopharynx: submucosal extension superiorly through the skull base foramina, laterally through the parapharyngeal and pterygoid spaces, anteriorly into the nasal cavity and maxillary sinuses, and posteriorly along the clivus.
The CTV54-59.4 for the primary begins with a 10 mm expansion around the GTV, then adds anatomically defined regions of risk. The entire nasopharyngeal mucosal space must be included. The soft palate is incorporated, as is the posterior nasal cavity — extending at least 5 mm anterior to the choana. The posterior portions of the maxillary sinuses are included to cover the pterygopalatine fossae and the V2 pathway, as is the posterior ethmoid sinus complex.
Skull base foramina — specifically the foramen ovale (V3), foramen rotundum (V2), and foramen lacerum — must be included in the CTV. These represent the highways for perineural spread into the middle cranial fossa. For T3-4 disease, the cavernous sinus and Meckel’s cave are added, reflecting the higher probability of intracranial perineural extension. The pterygoid plates and parapharyngeal space are included bilaterally. The sphenoid sinus is included partially (the posterior half) for T1-2 disease and entirely for T3-4 disease. The clivus follows a similar tiered approach: the posterior third for cases without bony invasion, the entire clivus when invasion is present or suspected on MRI.
These anatomic boundaries reflect decades of pattern-of-failure analyses. Recurrences at the skull base or along cranial nerve pathways carry devastating morbidity, and retreatment options in this region are severely limited. The use of SBRT for head and neck recurrences is an option in selected cases, but prevention through adequate initial coverage remains the preferred strategy.
Nodal Target Volumes: Bilateral Coverage Strategy

NPC has the highest rate of bilateral nodal involvement among all head and neck squamous cell carcinomas. Bilateral neck irradiation is therefore standard regardless of clinical nodal status. The CTV54-56 for the neck includes bilateral retropharyngeal nodes (a critical and often underappreciated station), levels IB, II, III, IV, and V.
Certain modifications are acceptable for early-stage disease. Level IB may be omitted in N0 patients without anterior extension of the primary into the nasal cavity or oral cavity. The low neck (level IV, supraclavicular fossa) may also be omitted for truly N0 patients, though many institutions prefer to include it given the modest additional volume. Level V — bordered posteriorly by the anterior edge of the trapezius muscle, and inferiorly by the fat plane posterior to the clavicular head — requires careful contouring, particularly in the context of advanced nodal disease. The approach to level V coverage shares methodology with laryngeal cancer delineation and hypopharyngeal cancer contouring, though the retropharyngeal component is unique to NPC.
The PTV for nodal volumes is generated with a uniform 3 mm expansion from the CTV. Unlike the primary site, where PTV reductions near the brainstem or optic apparatus are common, the nodal PTV rarely requires compromise — the neck is surrounded by relatively radiation-tolerant soft tissue, and full margin expansion is maintained.
Dose Prescription Tables and PTV Margins
| Volume | Primary Definition | Nodal Definition | PTV Margin | Dose |
|---|---|---|---|---|
| GTV70 | All gross disease on PE + imaging; skull base invasion; perineural spread on MRI | Nodes ≥1 cm short axis, necrotic nodes, FDG-avid nodes; contour doubtful nodes as GTV | — | — |
| CTV70 | GTV + 3–5 mm; 0 mm where GTV = CTV at bone/fascia; favor ipsilateral optic coverage, protect contralateral | GTV + 3–5 mm; small nodes may receive 63–66 Gy | Primary: 3–5 mm (compromise near brainstem/cord); Neck: 3 mm | 2.0–2.12 Gy/fx to 69.96–70 Gy in 33–35 fx |
| PTV70 | CTV70 + 3–5 mm (0 mm posteriorly near brainstem acceptable) | CTV70 + 3 mm | — | 69.96–70 Gy |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 1.1)
| Volume | Primary Subclinical Coverage | Nodal Subclinical Coverage | PTV Margin | Dose |
|---|---|---|---|---|
| CTV54-59.4 (Primary) | GTV + 10 mm + entire nasopharynx, soft palate, posterior nasal cavity (≥5 mm from choana), posterior maxillary sinuses (pterygopalatine fossae/V2), posterior ethmoid, skull base foramina (ovale, rotundum, lacerum), cavernous sinus/Meckel’s cave (T3-4), pterygoid & parapharyngeal spaces, sphenoid sinus (half for T1-2, whole for T3-4), clivus (1/3 if no invasion, whole if invaded) | — | 3–5 mm (0 mm near critical structures) | 35 fx: 1.6–1.7 Gy/day; 33 fx: 1.64–1.8 Gy/day |
| CTV54-56 (Neck) | — | Bilateral RP nodes, levels IB, II, III, IV, V. Level IB omittable if N0; low neck omittable if N0 | 3 mm | 54–56 Gy |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 1.2)
For sequential (non-SIB) approaches, the subclinical volume receives 50–54 Gy in the initial phase, followed by a cone-down boost of 16–20 Gy to the gross disease volume, yielding a total of 70 Gy. SIB techniques deliver all dose levels simultaneously, which is the predominant approach in modern IMRT practice for NPC.
Skull Base Anatomy: Foramina, Clivus, and Cavernous Sinus
The skull base is where NPC delineation either succeeds or fails. Three foramina deserve specific attention. The foramen ovale transmits the mandibular division of the trigeminal nerve (V3) and lies posterolateral to the lateral pterygoid plate. The foramen rotundum carries the maxillary division (V2) and opens into the pterygopalatine fossa anteriorly. The foramen lacerum, situated at the junction of the petrous apex, sphenoid body, and basilar occipital bone, represents a pathway to the internal carotid artery and cavernous sinus.
All three foramina must be included in the CTV54-59.4 for every NPC patient. When there is evidence of perineural disease on MRI, these pathways are escalated to the CTV70. The cavernous sinus and Meckel’s cave are added to the intermediate CTV for T3-4 disease.
The clivus deserves particular attention. This midline bone structure extends from the dorsum sellae superiorly to the foramen magnum inferiorly, and it is a frequent site of NPC invasion. For T1-2 tumors without evidence of clival invasion, the posterior third of the clivus is included in the subclinical CTV. When clival invasion is present or strongly suspected on MRI, the entire clivus must be included.
The pterygopalatine fossa connects the nasopharynx to the orbit (via the inferior orbital fissure), the middle cranial fossa (via the foramen rotundum), and the oral cavity (via the greater palatine canal). Including the posterior maxillary sinus walls in the CTV ensures coverage of this fossa and the V2 pathway traversing it.
Advanced and Recurrent Disease: T4 Considerations
T4 NPC presents the greatest contouring challenge. By definition, T4 disease involves intracranial extension, cranial nerve involvement, hypopharyngeal extension, orbital involvement, or extensive soft tissue infiltration. These patients require the most expansive subclinical volumes: the entire sphenoid sinus, the entire clivus, bilateral cavernous sinuses, and Meckel’s caves bilaterally.
The key principle is dose compromise at the PTV level, not the CTV level. If the CTV70 abuts the brainstem, the PTV70 may be reduced to 0 mm posteriorly, accepting that the brainstem surface will receive near-prescription dose. Modern IMRT optimization with dose painting can achieve steep gradients in this region, but the planner must be explicitly informed of where compromise is and is not acceptable.
For T4N2 presentations, level V coverage becomes critical, extending posteriorly to the anterior border of the trapezius and inferiorly to include the fat plane posterior to the clavicular head. The retrostyloid space must be meticulously contoured, particularly when retropharyngeal nodes are involved.
Adaptive Replanning and MRI-Guided Response Assessment
NPC is among the most responsive solid tumors to chemoradiation, and significant volumetric regression occurs during the treatment course. A mid-treatment MRI obtained around fraction 15–20 frequently demonstrates substantial GTV shrinkage, which can alter the spatial relationship between the tumor and critical structures — most notably the optic chiasm, brainstem, and temporal lobes.
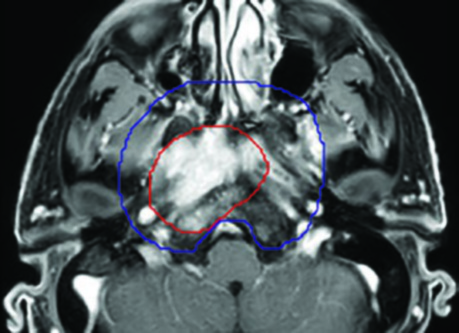
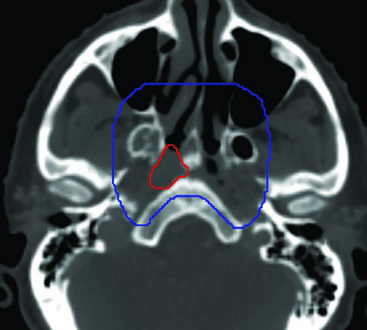
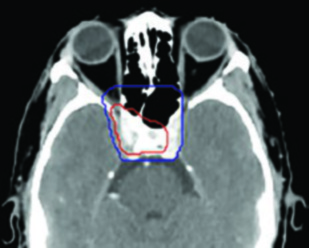
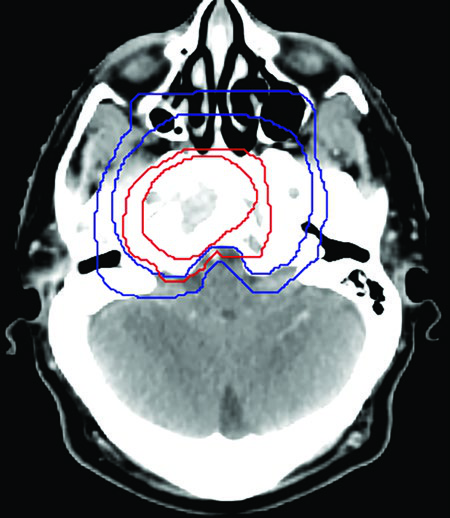
Adaptive replanning based on mid-treatment imaging is increasingly adopted. The primary indication is GTV shrinkage that creates a new gap between the tumor and a previously abutting organ at risk. In the illustrated case, a cT3N2 NPC demonstrated significant regression away from the optic chiasm at mid-treatment, permitting a replan that maintained full CTV70 coverage while reducing the chiasm maximum dose.
Weight loss and changes in body contour are additional indications for replanning. NPC patients receiving concurrent cisplatin frequently lose significant weight, altering the external contour and potentially shifting the dose distribution. A second CT simulation with re-optimization may be necessary when weight loss exceeds 5–7% of baseline body mass.
Key References and Final Remarks
The contouring principles described here are grounded in the consensus guidelines by Lee AW et al. (Radiotherapy and Oncology, 2018;126(1):25-36), the RTOG 0225 experience reported by Lee N et al. (Journal of Clinical Oncology, 2009;27(22):3684-90), and the NRG HN001 protocol.
Nasopharyngeal carcinoma target delineation is a discipline where attention to anatomic detail translates directly into clinical outcomes. The skull base foramina, the retropharyngeal nodal compartment, the perineural pathways along V2 and V3, and the tiered approach to sphenoid and clival coverage — each of these elements demands deliberate, case-by-case evaluation. No contouring atlas can substitute for correlation with the diagnostic MRI, the endoscopic findings, and the clinical context. For the complete overview of contouring methodology, refer to our complete guide to target volume delineation.