

Fractionated radiotherapy assumes that the patient’s anatomy remains sufficiently stable throughout the treatment so that the plan generated in the simulation CT maintains dosimetric validity. In practice, this premise fails to varying degrees: mass loss, tumor regression, variations in visceral filling and accumulated postural changes redistribute the geometric relationships between target, organs at risk and beams. Adaptive radiotherapy (RTA) responds to these variations by partially or completely replanning the treatment during the course, based on images acquired in the treating unit itself or in an adjacent system. Dose recalculation over these images — not just geometric verification — is what transforms RTA from an empirical fit into a dosimetrically traceable tool.
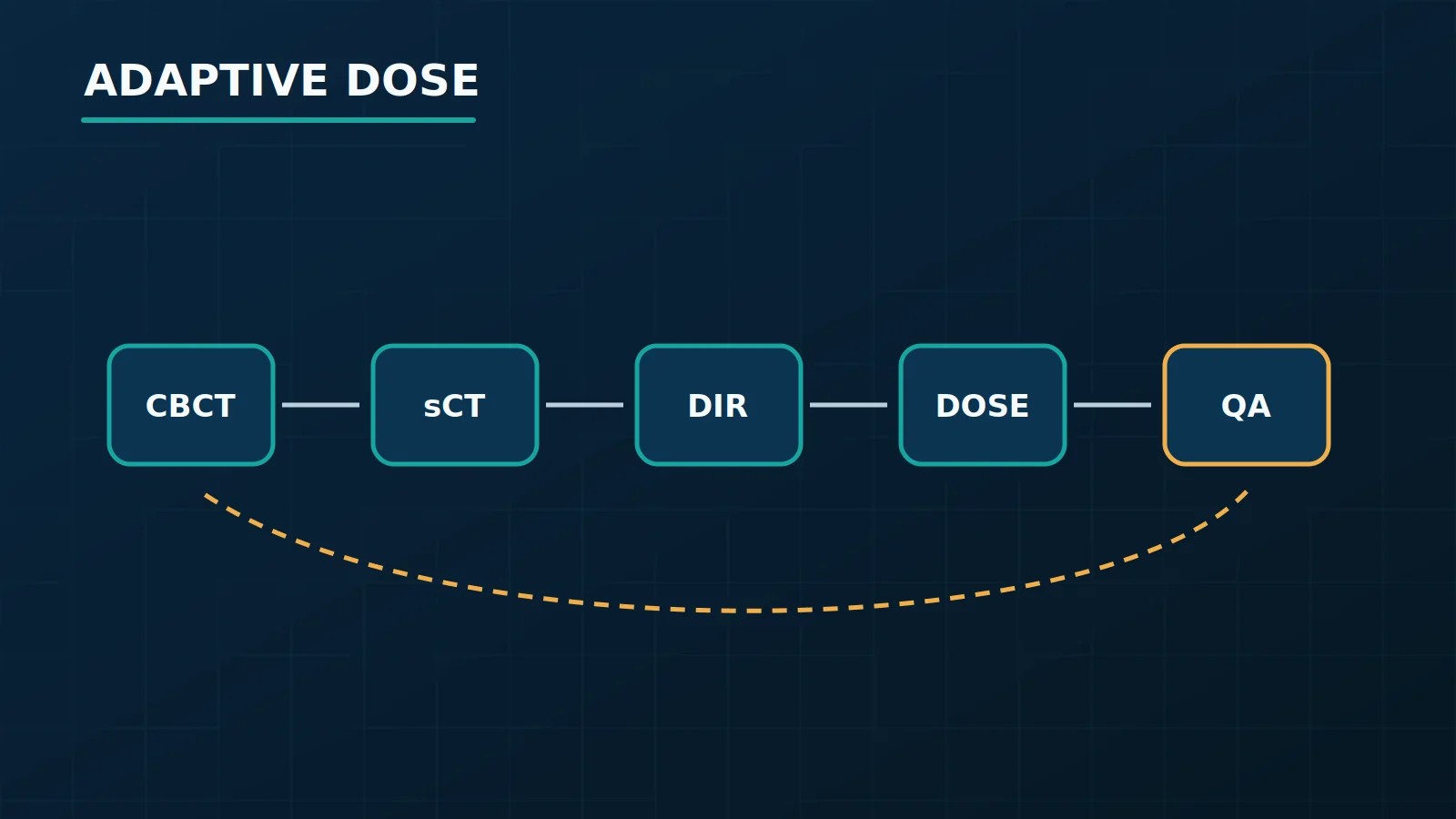
The central challenge is that the images available throughout treatment, notably cone-beam tomography (CBCT), were not designed for dose calculation: their Hounsfield values (HU) are systematically affected by scattering, beam hardening and field of view truncation in a way that is qualitatively different from diagnostic or simulation CT. Overcoming this limitation requires processing chains that encompass HU correction or replacement, deformable image registration (DIR), synthetic CT (sCT) generation, and eventually dose accumulation throughout the fractions. Each step introduces uncertainties that propagate to the final dose estimate. A state-of-the-art review published with support from NRG Oncology Sonke et al. catalogs technical approaches and validation requirements; a 2024 update Yang et al. mapped active clinical flows and still open gaps; and a review dedicated to adaptive proton therapy Albertini et al. discusses how sensitivity to beam range makes recalculation even more critical in this modality.
In this article we describe the physics and workflows involved in dose recalculation in CBCT and sCT, differentiating what is an established physical description, implementation in commercial products and clinical validation evidence. The objective is to provide the medical physicist and radiation oncologist with a technical reference to critically evaluate the available solutions and the safety criteria necessary for their adoption.
In this Article
- 1. What adaptive recalculation needs to represent
- 2. Why raw CBCT is not equivalent to planning CT
- 3. HU correction, deformation and synthetic CT
- 4. Deformable registration and dose accumulation
- 5. Online calculation: speed versus fidelity
- 6. Patient-specific QA and safety controls
- 7. Practical criteria for deciding when to adapt
- 8. Frequently Asked Questions
- 9. References
What adaptive recalculation needs to represent
A dose calculation engine transforms a volumetric representation of the patient’s electron or mass density into an absorbed dose distribution. Pencil Beam, AAA, Acuros XB, and Monte Carlo engines differ in how they model scattering, electron transport, and interfaces. The distinction between dose to medium and dose to water It is implementation dependent and needs to be documented in the recalculation because it affects comparability between distributions and clinical criteria.
For adaptive recalculation, TPS needs four fundamental elements: (1) a reliable geometric representation of the anatomy of the day, including position and shape of tumor and organs at risk; (2) HU — or density equivalent — values accurate enough for the dose algorithms involved; (3) contours updated or propagated via DIR, on which dosimetric metrics will be evaluated; and (4) traceability to the original plan, so that the accumulated dose can be compared to the prescribed dose with a consistent magnitude and unit.
The required precision is not uniform across the volume: regions of high heterogeneity — air-tissue interfaces, cortical bone, and metallic prostheses — are more sensitive to HU uncertainties than homogeneous soft tissues. This has direct implications for which clinical sites recalculation on CBCT or sCT is dosimetrically sufficient and where method limitations become clinically relevant enough to require alternative strategies or additional caution.
Why raw CBCT is not equivalent to planning CT
Planning CT is acquired with fan-beam geometry (fan-beam), equalization filters (bowtie) and protocols optimized for HU linearity with respect to electron density; this relationship is the basis of commissioning of TPS. CBCT operates with cone geometry, flat-panel detectors, and longer acquisition times — conditions that amplify the scattering contribution to the detected signal.
The practical consequences for dose calculation are well documented:
- Nonlinearity of HU: soft tissue values in CBCT differ systematically from their counterparts in simulation CT, with variations depending on patient size, acquisition protocol, position in the reconstructed volume and equipment manufacturer.
- Beam hardening artifacts (beam hardening): produce bands of HU under- and overestimation, particularly pronounced near dense bone structures; the cortical bone of the pelvis and jaw are recurrent examples in clinical CBCT.
- Truncation of the field of view (FOV): in patients with a diameter larger than the reconstructed FOV, the extension algorithms introduce additional uncertainties in the peripheral HU.
- Lower signal-to-noise ratio: higher noise than in the simulation CT affects both the dose calculation and the quality of the subsequent DIR.
- Absence of standardized dosimetric calibration: CBCT manufacturers do not, in general, provide validated HU-density relationships for dosimetric use with the same degree of traceability as diagnostic CT manufacturers.
The sum of these factors prevents the assumption that raw CBCT is dosimetrically equivalent to the planning CT. Direct use can only be accepted within a local acquisition, calibration and validation protocol that demonstrates sufficient performance for the site and algorithm evaluated.
HU correction, deformation and synthetic CT
Three main strategies are used to overcome the dosimetric inadequacy of raw CBCT, with distinct characteristics, dependencies and failure points:
1. Correction by conversion table (LUT) or scaling
Maps CBCT HU to planning CT equivalent HU via a table derived from phantoms or image pairs clinics. More sophisticated variants apply regional correction or correction adapted to the patient’s size. The fundamental limitation is structural: the LUT is derived under average conditions and does not capture inter-patient variations or local anatomy dependencies. It may be acceptable for low-heterogeneity sites with wide margins, but is unsuitable for high-precision SBRT in regions with strong density variation.
2. DIR with density propagation from the reference CT
Deformably register the planning CT to the day’s CBCT and use the deformation field to transport the HU from the reference CT to the current geometry. This approach inherits the dosimetric quality of the simulation CT, but transfers the error to the DIR: regions where registration fails — for example, when there is variation in tumor volume without structural correspondence in the original CT — generate incorrect densities that do not necessarily trigger visual alerts. The 2024 revision specifically discusses scenarios where this failure is clinically significant.
3. Synthetic CT (sCT) by machine learning
Neural networks trained on CBCT/CT pairs can improve fidelity over simple LUTs. In the context of MRI-linac, different products use density assignment, warped reference CT, or sCT, because MRI does not provide electron density directly. For CBCT, the adopted method must be described and validated by product, version and clinical site.
The distinction between method description and validation evidence is critical in this context: an sCT with an acceptable mean HU error in a phantom or in a development cohort does not guarantee equivalent dosimetric performance in patients with atypical anatomies, extreme weight variations or metallic implants. THE NRG state of the art establishes validation requirements that include dosimetric comparison with planning CT in cohorts representative of the clinical sites of intended use.
| Method | Implementation complexity | Dependence on DIR | Major risk |
|---|---|---|---|
| LUT / global scaling | Low | None | Systematic errors in atypical anatomies and regions of high heterogeneity |
| DIR + CT HU propagation | Moderate | High | DIR failure on topology changes or large local deformations |
| sCT by machine learning (CBCT) | High (training and validation) | Partial | Generalization outside the training distribution; atypical artifacts |
| sCT from MRI (MR-Linac) | High | Low to moderate | MRI artifacts, metallic implants, intrafraction movement |
Deformable registration and dose accumulation
DIR is transversal to almost all stages of RTA: propagates contours from the planning CT to the images of the day, generates deformation fields used in propagation of HU or in the generation of sCT and, in the dose accumulation function, transforms dose distributions of different fractions to a common coordinate system.
Dose accumulation by DIR assumes that the deformation field $\mathbf{u}(\mathbf{x})$ faithfully represents the mapping of each voxel in the reference image to its counterpart in subsequent images. This hypothesis fails in well-defined scenarios:
- Topological changes: tumor that regresses completely or cavity that appears — there is no anatomical correspondence for new or disappeared regions;
- Sliding surfaces (sliding interfaces), such as the lung-chest wall interface or mobile intestine: algorithms based on the smoothness of the deformation field underestimate kinematically real discontinuities;
- Regions of low image contrast: the DIR converges to solutions that are locally plausible, but not necessarily correct from an anatomical point of view;
- Non-biomechanical deformations: post-radiotherapy edema or fluid accumulation do not obey the restrictions implicit in most commercial algorithms.
For protons, where dose distribution is even more sensitive to density variations along the beam path—in particular Bragg peak shift—the Adaptive Proton Therapy Review describes additional DIR validation requirements and scenarios in which dose accumulation produces reasonably reliable estimates versus where uncertainties are unacceptably large to support clinical decisions.
DIR validation is a field in itself: AAPM TG-132 establishes metrics and test flows that include use of deformable phantoms and target registration error (TRE) analysis. A frequently underestimated limitation is that low TRE at explicit control points does not guarantee dosimetric accuracy in the regions between them — especially in areas of low density of recognizable anatomical landmarks.
| Clinical scenario | DIR reliability | Expected impact on accumulated dose |
|---|---|---|
| Weight variation without topological change | Moderate to high | Moderate, if DIR is validated for site |
| Tumor regression with volume collapse | Low to moderate | High — regions without anatomic correspondence |
| Pleural slip / lung-wall interface | Low without dedicated algorithm (sliding) | High on the interface; can propagate to target |
| Rectal/vesical filling variation (prostate) | Low | High — topology changes between fractions |
| Post-dose edema or fluid accumulation | Low | High — deformation without direct biomechanical basis |
Online calculation: speed versus fidelity
The RTA online — in which replanning occurs with the patient on the table, between image acquisition and the start of treatment — imposes time restrictions that directly influence the choice of dose calculation engine. The time windows available in commercial integrated systems are tens of minutes in total, but the effective time for calculation is only a fraction of this range, competing with image acquisition, HU correction or sCT generation, DIR, contour propagation, dosimetric evaluation, and clinical approval.
The calculation engines used in online flows involve explicit commitments:
- Pencil Beam andkernel methods: can offer low latency, but the validation domain needs to cover the heterogeneities and adaptive image used in the flow.
- LBTE solvers: represent transport more explicitly, but speed, dose convention, and online flow support are product and version dependent.
- Monte Carlo accelerated: can represent heterogeneities with high fidelity, but statistics, beam model, hardware and modality need to be considered. GPUMCD is not a generic term for proton calculation.
The commissioning of a calculation engine for use in online RTA goes beyond validation in reference fields. It should include calculation speed scenarios and image types—corrected CBCT or sCT—that will be used clinically, with tolerances defined specifically for each combination of site, algorithm, and input image. It is not valid to transfer commissioning results from one input image type to another without specific validation.
An important practical distinction: Commercial integrated RTA systems implement proprietary flows that combine sCT generation, DIR, dose calculation, and approval interface in a unified environment. Validation of these specific implementations is not transferable directly from publications that tested the components in isolation — each institution must conduct its own clinical commissioning in the installed environment, with test patients representative of the intended use sites.
Patient-specific QA and safety controls
Adaptive plan QA differs from conventional QA in relevant structural aspects. In RTA offline, it is possible to export the adapted plan to an independent verification system and perform measurements before delivery — the flow is analogous to conventional IMRT/VMAT QA, with the difference that the plan can change with each fraction or group of fractions, requiring more frequent and agile QA capacity than usual.
At RTA online, the time available for independent QA before delivery is severely restricted. Strategies adopted include:
- Verification by automated secondary calculation: an independent algorithm — often Monte Carlo simplified or analytical model — recalculates the adapted plan dose based on the same images, and agreement with TPS is verified within predefined tolerances before final approval.
- DVH Automatic consistency controls: automatic comparison of adapted plan metrics with the reference plan, with configurable triggers for maximum differences in D95% of target, Dmax in critical OAR and projected cumulative dose.
- Geometric verification of propagated contours: visual and, when possible, metric confirmation that the contours generated by DIR are clinically acceptable before dose calculation — an often underestimated step in online flow automation.
- Documented fallback plan: the original plan or a previously adapted and approved plan must be available for immediate delivery if the day’s plan does not pass controls, without clinical delay.
- Formal and traceable clinical approval: The radiation oncologist explicitly reviews and approves the adapted plan before each fraction in which it differs significantly from the reference plan.
The definition of tolerances and actions for online RTA is not uniformly standardized at the level of international guides to the same degree as conventional IMRT QA. The NRG revision discusses specific QA requirements by technology and site, but emphasizes that tolerances must be derived locally based on validation of the installed system.
An often underestimated failure scenario is the silent propagation of errors from DIR to dose calculation: a visually plausible strain field can produce incorrect densities in critical regions without triggering any automatic alerts. Systematic visual inspection of sCT or corrected densities — especially in regions of high heterogeneity and at target-OAR interfaces — before each approval cannot be fully replaced by automatic metrics.
Practical criteria for deciding when to adapt
The decision to adapt involves three simultaneous dimensions: detectable and measurable anatomical change; clinically relevant dosimetric impact resulting from this change; and availability of infrastructure to safely carry out replanning within the available clinical time. Not every anatomical change justifies redesign; Not every replanning improves the outcome compared to following the original plan, especially when the original margins were sized to absorb some of the expected variability.
Common anatomical triggers:
- Body weight variation beyond an institutionally defined threshold in relation to the simulation weight — often used in the head and neck;
- Visible tumor regression with risk of inadequate target coverage margin;
- Modification of rectal or bladder filling beyond institutional volumetric thresholds — prostate and pelvis in general;
- Pleural effusion, atelectasis or variation in lung aeration that alters the beam-RAO relationship;
- Variation in position or volume of lymph nodes included in the target volume.
Dosimetric triggers when recalculation is feasible:
- Drop in target coverage with D95% of GTV or CTV below the threshold defined in the protocol;
- Projected increase in cumulative dose in critical OARs above established tolerances, such as cumulative spinal dose or head and neck brainstem dose.
Considerations by clinical site:
- Head and neck: high degree of anatomical change throughout treatment — weight loss, tumor regression, edema reduction — and site with the greatest volume of published evidence on the benefit of RTA; it also presents greater complexity of IRD due to adjacent bone and mucosal structures.
- Lung (SBRT/SABR): variation in interfraction tumor position, lung collapse and pleural effusion are the main drivers; Limitations of DIR due to pleural slip are relevant to dose accumulation.
- Prostate: daily variation in rectal and bladder filling motivates online ART approaches; the magnitude of the adaptive benefit depends on the margins originally used.
- Uterine cervix: large uterine geometric variation throughout the treatment; well-established candidate for RTA, with adaptive brachytherapy as a long-standing conceptual reference.
- Protons (any site): sensitivity to beam range amplifies the dosimetric impact of any anatomical changes along the beam path, including density variations in structures proximal to the target, making the recalculation indication more frequent than in equivalent photons, as discussed in the review of adaptive protons.
The absence of an integrated RTA platform does not impede adaptive practice. RTA offline with periodic recalculation — weekly or in response to clinical triggers — is feasible in most DIR-compliant CBCT and TPS services, as long as the approval flow is rigorous and QA controls are documented in operating procedure.
Frequently Asked Questions
Is it safe to use CBCT directly for dose calculation without correction?
It should not be assumed to be safe. Direct use requires local evidence that the CBCT protocol maintains a sufficient density-to-image ratio for the site, field of view and algorithm evaluated. In the absence of this validation, an also validated density correction or replacement chain must be used.
Is synthetic CT generated by neural network equivalent to planning CT for dose calculation?
It depends on the quality of the network, the anatomical site and the representativeness of the validation population. Under well-validated conditions and for anatomies within the training distribution, sCT can achieve dosimetric performance comparable to planning CT on aggregated cohort metrics. Outside of these conditions—patients with metallic implants, atypical anatomies, or atypical acquisition artifacts—sCT fidelity may be insufficient to the extent that it is not always detectable by automatic controls. Validation must be conducted institutionally for each clinical site and acquisition protocol; results from other centers with different equipment are not directly transferable.
Which dose calculation engine is best suited for online RTA?
There is no universal answer. The choice depends on the calculation time available on the installed platform, the clinical site and the degree of anatomical heterogeneity, the complexity of the plan and acceptable dosimetric tolerances. Engines based on LBTE (Acuros XB) and GPU-accelerated Monte Carlo (GPUMCD) offer greater physical fidelity across inhomogeneities, but can be slower than Pencil Beam variants in less optimized configurations. commissioning must explicitly document which speed and accuracy setting combinations have been validated for clinical use on the installed system.
Is DIR reliable enough for clinical dose accumulation?
DIR can support the decision when it has been validated for the site and type of deformation. Large deformations, slippage and topological changes increase uncertainty. The accumulated dose must be presented as a record-dependent estimate, not as a value automatically equivalent to the dose calculated directly in each anatomy.
How to integrate adaptive plan QA with the restricted time of the online flow?
The most adopted strategy combines verification by automated secondary calculation with predefined and validated tolerances, mandatory visual inspection of propagated contours and dose distribution by the physicist and physician, and availability of an approved fallback plan for immediate delivery if the day’s plan does not pass controls. The definition of secondary calculation tolerances and DVH metrics acceptance thresholds must occur during the system’s commissioning , based on the specific uncertainties of the installed processing chain — not from values published by other centers without local verification.


