

Theranostics has moved from a niche therapy to the center of nuclear medicine. That was the dominant message at the 2026 annual meeting of the Society of Nuclear Medicine and Molecular Imaging (SNMMI) in Los Angeles. New theranostics agents filled the scientific sessions, while a fresh generation of PET radiotracers signaled that the field is advancing quickly toward personalized medicine.
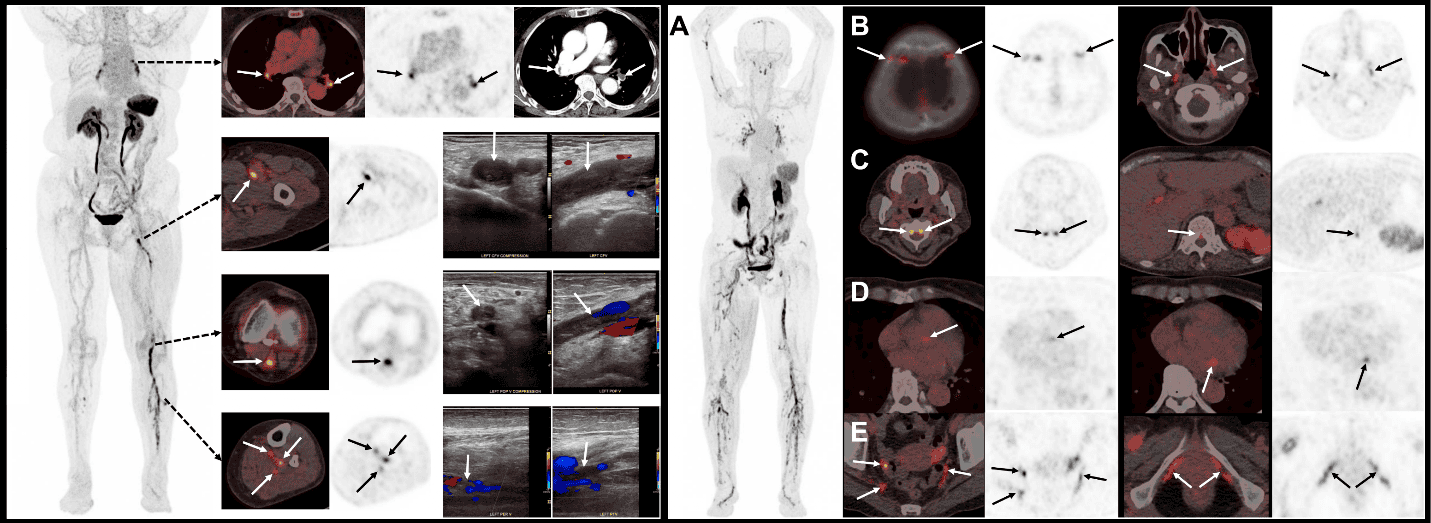
Image of the Year: PET for deep vein thrombosis
The Image of the Year award went to South Korean researchers who used the 18F-GP1 radiotracer on PET/CT to identify acute lower-extremity deep vein thrombosis (DVT). In a study of 46 symptomatic patients, the tracer showed high diagnostic accuracy for detecting clots not only in the thigh but also in the calf — a region that is traditionally harder to assess. It also achieved a high detection rate for pulmonary embolism occurring together with DVT.
This molecular approach speaks directly to what we have covered about the role of artificial intelligence in pulmonary embolism detection, where imaging and algorithms combine to speed up the diagnosis of potentially fatal events.
Abstract of the Year: brain metabolism and Alzheimer’s response
The Abstract of the Year went to a study that used PET to link brain metabolism patterns to the effectiveness of Alzheimer’s disease therapies. UCLA researchers performed FDG-PET brain scans on 124 patients being considered for anti-amyloid therapy. Those whose scans suggested Alzheimer’s and who received treatment had higher cognitive scores at one year compared with patients whose PET showed no evidence of the disease.
The finding reinforces the trend of using molecular imaging as a selection and response biomarker — a path similar to the one explored in AI-based mapping of cerebral blood flow and Alzheimer’s with MRI, where neuroimaging helps define who benefits from each therapy.
What theranostics is and why it is growing so fast
Theranostics combines diagnosis and therapy in a single concept: a pair of molecules binds to the same biological target — one labeled with a positron-emitting isotope for imaging (PET) and another with a particle emitter (beta or alpha) for treatment. The scan that locates the disease also confirms that the target is present before irradiating it. The most established example is PSMA in prostate cancer, where gallium-68 performs the imaging and lutetium-177 delivers the therapeutic dose.
This rapid growth rests on three factors: the approval of radiopharmaceuticals such as lutetium-177 PSMA, expanded isotope production and the entry of artificial intelligence into dosimetry. Together they make it feasible to treat tumors once considered refractory, with lower toxicity than conventional chemotherapy.
Scientific highlights: from kidney to prostate
The meeting delivered a stream of new tracers and strategies. Among the highlights presented:
- FDG-PET/CT scans showed that patients who underwent bariatric surgery had metabolic changes across multiple organs that correlated with improved clinical markers.
- The new tracer gallium-68 RCC78 detected clear cell renal cell carcinoma and identified additional metastatic lesions missed by standard imaging.
- A first-in-human study with the tracer carbon-11 nevanimibe was presented for imaging overactive adrenal glands.
- In metastatic neuroendocrine tumors, a new peptide receptor radionuclide therapy (PRRT) using actinium-225 DOTA-LM3 showed promise.
- PSMA-PET scans showed that prostate cancer patients with just one to five bone metastases had far worse outcomes than those with none.
- A dual-tracer PET approach during cancer treatment detected both tumor progression and cardiac inflammatory response.
- An AI algorithm using pre-therapy PET/CT data predicted radiation dose in lutetium-177 PSMA treatment for prostate cancer.
Why theranostics matters in practice
The logic of theranostics — using the same molecular target to diagnose and to treat — reshapes the imaging department workflow. PET stops being only a staging exam and starts guiding patient selection, dose calculation and response monitoring. For radiologists and nuclear medicine physicians, this underscores the need for integrated imaging and dosimetry protocols, plus structured reports that clearly communicate the parameters used in each therapeutic cycle.
In practice, services planning to offer lutetium-177 or actinium-225 therapy will need quality PET/CT, rigorous radiopharmaceutical quality control and teams trained to read imaging as a treatment guide — not just as a standalone diagnosis. Centers will also need to align radiopharmacy logistics, regulatory clearance and reimbursement pathways so that these therapies reach patients without prohibitive delays, while building referral networks between diagnostic imaging units and treatment centers.
Outlook: toward personalized medicine
The takeaway from SNMMI 2026 is clear: theranostics has evolved from a last-resort option into a pillar of precision oncology. The proliferation of tracers beyond FDG extends molecular imaging into prostate, kidney, adrenal and central nervous system disease. As AI enters dosimetry and response prediction, each patient is likely to receive an increasingly individualized plan. Anyone following prostate cancer screening and management can already see how this molecular ecosystem is becoming the new standard of care.
Source: The Imaging Wire


