

Target volume delineation for oral cavity cancers demands detailed anatomical knowledge and precise imaging correlation. Tumors arising from the oral tongue, buccal mucosa, floor of mouth, gingiva, hard palate, and retromolar trigone each exhibit distinct patterns of spread. Defining the correct CTVs is what ultimately balances tumor control against functional preservation. This article details the delineation guidelines, dose prescriptions, and volume definitions for both definitive and postoperative treatment, based on Target Volume Delineation and Field Setup, 2nd edition.
For a comprehensive overview of all anatomical sites covered in this series, see our complete guide on target volume delineation and field setup.
In This Article
- Imaging Evaluation and Simulation Setup
- Definitive Treatment Target Volumes
- Postoperative Treatment Target Volumes
- Site-Specific Contouring Guidelines
- Clinical Case: Oral Tongue Carcinoma
- Clinical Case: Buccal Mucosa
- Clinical Case: Retromolar Trigone
- Clinical Case: Gingiva with Bone Invasion
- Clinical Case: Buccal Mucosa with Extranodal Extension
- Clinical Case: Floor of Mouth
Imaging Evaluation and Simulation Setup
Every patient with oral cavity cancer should undergo a comprehensive oral examination, biopsy, and staging imaging before radiation planning. Computed tomography (CT) with intravenous contrast is the standard for evaluating local tumor extent and cervical lymph node involvement. CT excels at detecting invasion of the mandible, maxilla, and pterygopalatine fossa — locations where the decision to include or exclude bony structures in the CTV fundamentally changes the treatment plan.
Magnetic resonance imaging (MRI) is superior to CT for evaluating soft tissue extension and perineural spread. In practice, when there is suspicion of inferior alveolar nerve or mandibular branch of the trigeminal nerve involvement, MRI is indispensable. PET-CT is useful for evaluating regional lymph nodes and ruling out distant disease, particularly relevant in advanced staging.
CT simulation with IV contrast should be performed with the patient supine, neck slightly hyperextended, using a five-point thermoplastic mask. A bite block can be placed to depress the tongue and protrude the lower lip while elevating the hard palate — a maneuver that displaces normal tissues away from the treatment volume. Radiopaque wire should mark surgical scars and drain sites. When extranodal extension is present or the scar is at risk, tissue-equivalent bolus ensures adequate surface coverage.
Definitive Treatment Target Volumes
In the definitive setting, three CTV tiers structure the prescription. The GTV70 encompasses all gross disease visible on physical examination and imaging. The CTV70 is identical to the GTV70, though a 5 mm margin — excluding bone — can be added when there is uncertainty regarding the full extent of gross disease.
The CTV59.4 (high-risk subclinical) must encompass the entire CTV70 and cover the entire anatomic subsite of origin. For an oral tongue cancer, the entire oral tongue is included. For buccal mucosa, the entire buccal mucosa. Additionally, nodal levels with pathologic involvement and adjacent ipsilateral or contralateral levels at high risk for subclinical disease are included.
The CTV54 (low risk) covers ipsilateral and/or contralateral uninvolved nodal levels at low risk for subclinical disease.
Definitive Treatment Volumes and Doses
| Target Volume | Definition and Description |
|---|---|
| GTV70 | Primary: all gross disease on examination and imaging. Neck: all gross nodal disease. |
| CTV70 | Same as GTV70; 5 mm margin (excluding bone) may be added if uncertainty regarding extent. |
| CTV59.4 | Primary: CTV70 + entire anatomic subsite. Neck: levels with disease + adjacent high-risk subclinical levels. |
| CTV54 | Ipsilateral and/or contralateral uninvolved nodal levels at low risk for subclinical disease. |
PTV70 = 69.96 Gy in 2.12 Gy/fraction; PTV59.4 = 59.4 Gy in 1.8 Gy/fraction; PTV54 = 54 Gy in 1.64 Gy/fraction. Alternative: 70 Gy in 2 Gy/fraction with sequential or simultaneous integrated boost. Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 6.1).
Postoperative Treatment Target Volumes
In the postoperative setting, the hierarchy shifts. The CTV66 covers regions of microscopically positive margins or extracapsular extension — situations that demonstrably raise the risk of local recurrence. The CTV60 encompasses preoperative gross disease, the entire operative bed, and the relevant anatomic subsite, along with high-risk nodal levels. The CTV54 follows the same logic as the definitive scenario: low-risk subclinical levels.
If gross residual disease is present, the GTV should be delineated separately. Postoperative doses are: PTV66 = 66 Gy in 2.2–2.0 Gy/fraction; PTV60 = 60 Gy in 2 Gy/fraction; PTV54 = 54 Gy in 1.8 Gy/fraction.
Postoperative Volumes and Doses
| Target Volume | Definition and Description |
|---|---|
| CTV66 | Primary: regions of soft tissue/bone invasion or microscopically positive margins. Neck: regions of extracapsular extension. |
| CTV60 | Primary: preoperative gross disease + entire operative bed + entire anatomic subsite. Neck: preoperative disease + operative bed + high-risk subclinical levels. |
| CTV54 | Ipsilateral and/or contralateral uninvolved nodal levels at low risk for subclinical disease. |
If gross residual disease: delineate GTV separately. PTV66 = 66 Gy in 2.2–2.0 Gy/fraction; PTV60 = 60 Gy in 2 Gy/fraction; PTV54 = 54 Gy in 1.8 Gy/fraction. Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 6.2).
Site-Specific Contouring Guidelines
Each subsite within the oral cavity has distinct lymphatic drainage patterns and local spread behavior, requiring specific adjustments to target volumes. The table below summarizes recommendations by site and stage, differentiating between high-risk and low-risk subclinical volumes. For well-lateralized tumors of the buccal mucosa, gingiva, or retromolar trigone, contralateral neck treatment may be omitted at the treating physician’s discretion. Hard palate tumors are typically of salivary origin (such as adenoid cystic carcinoma), and coverage of the trigeminal nerve tracks should be included — while neck coverage can often be omitted due to the low rate of nodal spread in these tumors.
Special attention for oral tongue tumors: level VI is a drainage site and its inclusion is strongly recommended, especially with node-positive disease. This recommendation extends to scenarios of extranodal extension, as discussed in our articles on larynx cancer delineation and hypopharyngeal carcinoma.
Site-Specific Guidelines Table
| Subsite | Stage | High-risk CTV (CTV59.4 or CTV60) | Low-risk CTV (CTV54) |
|---|---|---|---|
| Oral tongue, floor of mouth | T1–T4N0 | Tumor bed, entire oral tongue, base of tongue, bilateral levels I–IV at physician’s discretion | Bilateral levels I–IV at physician’s discretion. Prophylactic level VI when indicated. |
| T1–T4N1–3 | Same as above plus level VI nodal regions | Same as above plus level VI | |
| Buccal mucosa, retromolar trigone, hard palate, gingiva | T1–T2N0 | Tumor bed + ipsilateral levels I–IV at physician’s discretion | Ipsilateral levels I–IV at physician’s discretion |
| T3–T4N0 | Tumor bed + ipsilateral levels I–IV | Contralateral levels II–IV | |
| T1–T4N1–3 | Tumor bed + ipsilateral levels I–V or bilateral I–V if contralateral involved | Contralateral levels II–IV if uninvolved |
66 Gy for positive margins or extracapsular extension; 70 Gy for gross residual disease. For well-lateralized buccal mucosa/gingiva/retromolar trigone tumors, contralateral neck may be omitted. Hard palate: cover trigeminal nerve tracks; neck may be omitted. Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 6.3).
Clinical Case: Oral Tongue Carcinoma T3N2b
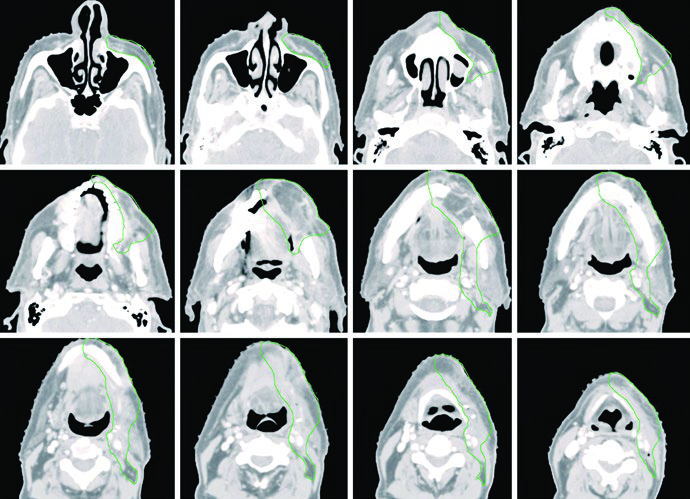
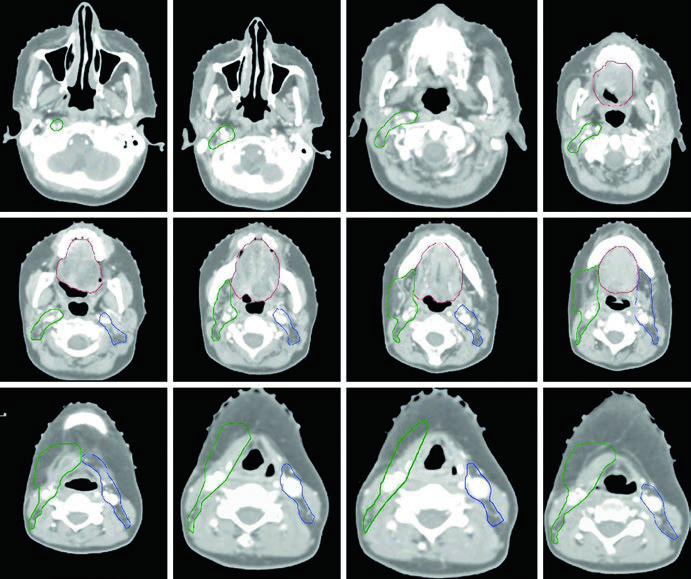
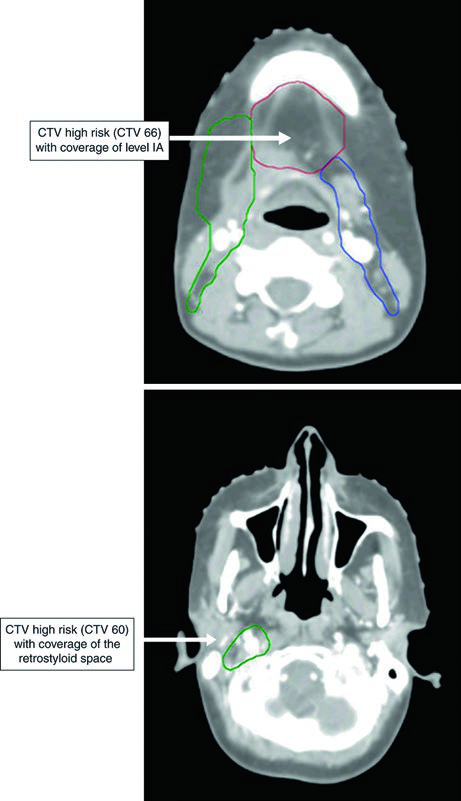
Figure 6.1 illustrates a patient with squamous cell carcinoma (SCC) of the oral tongue, pathologic stage T3N2b, status post-partial glossectomy with microscopically positive surgical margins. The CTV66 (red) encompasses the positive margin. The CTV60 (green) covers the entire operative bed, and the CTV54 (blue) includes the cervical nodal levels.
On the ipsilateral side, levels I through V are included. On the uninvolved contralateral side, levels I through IV. Level V coverage is recommended for oral tongue primaries, especially after surgical manipulation of the neck and with ipsilateral nodal disease. Level IA should be systematically covered for oral tongue tumors.
When there are concerns about soft tissue involvement, bolus and flash are recommended to provide adequate surface coverage. The ipsilateral retrostyloid space is at risk for nodal metastasis, particularly with level II involvement. Retropharyngeal nodes are at low risk and are not included. Level VI coverage is highly recommended for patients with node-positive disease.
Clinical Case: Buccal Mucosa T4aN0
Figure 6.2 shows a patient with SCC of the buccal mucosa, T4aN0, with minimal cortical bone invasion, status post-tumor resection with marginal mandibulectomy and left neck dissection. Surgical margins were widely clear. The CTV60 (green) covers the operative bed with ipsilateral neck levels I through IV.
The CTV extends cranially to the buccal-gingival sulcus and infratemporal fossa, caudally to the buccal-gingival sulcus and submandibular gland, anteriorly to at least the lip commissure, and posteriorly to the retromolar trigone. Bolus is placed on the skin to provide adequate high-risk CTV coverage. Ipsilateral parotid inclusion should be considered when clinically concerning. This pattern of volume extension is also relevant for sinonasal tumors, which share anatomical proximity.
Clinical Case: Retromolar Trigone T4aN2b
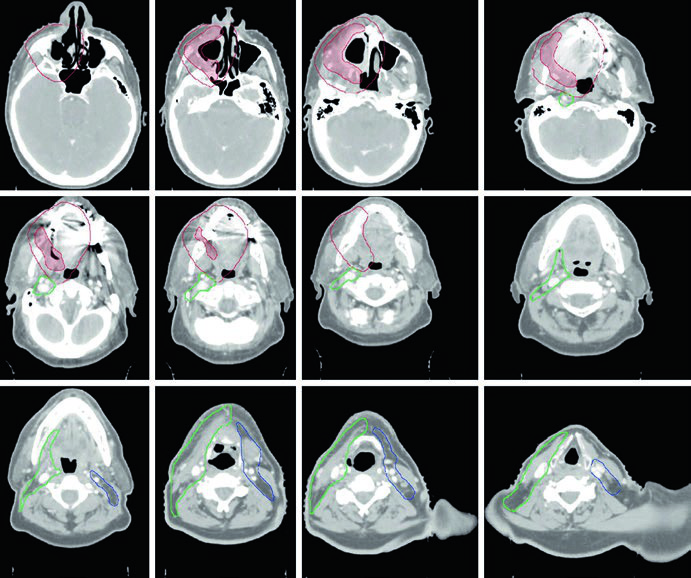
Figure 6.3 demonstrates SCC of the retromolar trigone, T4aN2b, with medial pterygoid involvement, status post-tumor resection with gross residual disease in the tumor bed and right neck dissection. The CTV70 (shaded red) is delineated based on operative findings along with pre- and postoperative imaging.
The CTV59.4 is shown in red (tumor bed region) and green (ipsilateral neck). The CTV54 (blue) includes contralateral neck levels IB through IV.
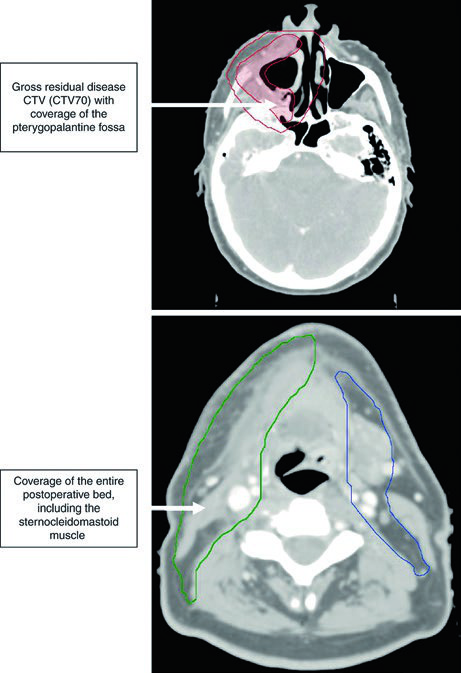
The pterygopalatine fossa serves as a gateway for tumor spread to the middle cranial fossa. Adequate coverage is essential when the pterygoid muscle is invaded. Postoperative tumor volumes must include the entire operative bed, using tissue inflammation and edema on the planning CT to delineate areas of surgical manipulation.
Clinical Case: Gingiva T4aN1 with Bone Invasion
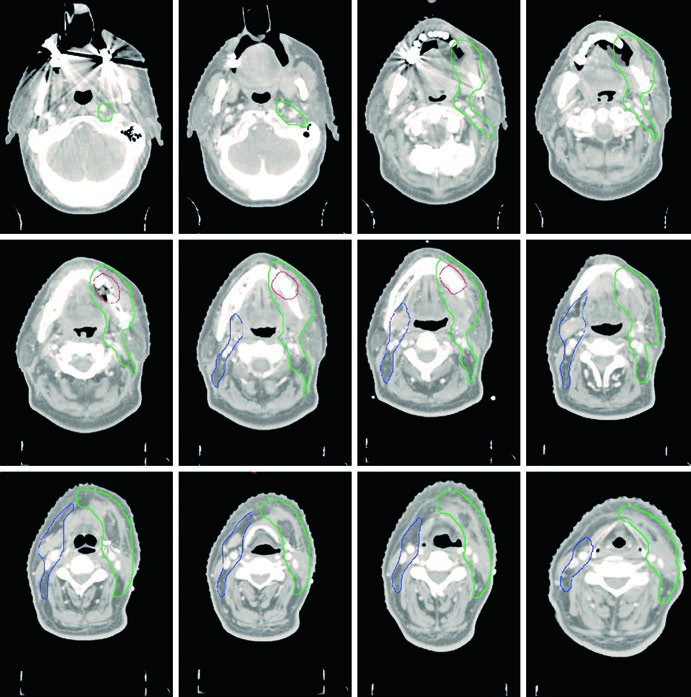
Figure 6.4 shows SCC of the gingiva, T4aN1, with bone invasion, status post-tumor resection with marginal mandibulectomy and left neck dissection. The CTV66 (red) covers the region of bone invasion. The CTV60 (green) includes the entire operative bed and ipsilateral levels I through IV.
The CTV54 (blue) covers contralateral levels I through IV. The decision to include the contralateral neck was based on node-positive disease (N1) and T4 staging — both factors that raise the risk of contralateral involvement. For well-lateralized gingival tumors with more favorable staging, this coverage could be omitted.
Clinical Case: Buccal Mucosa T2N3b with Extranodal Extension
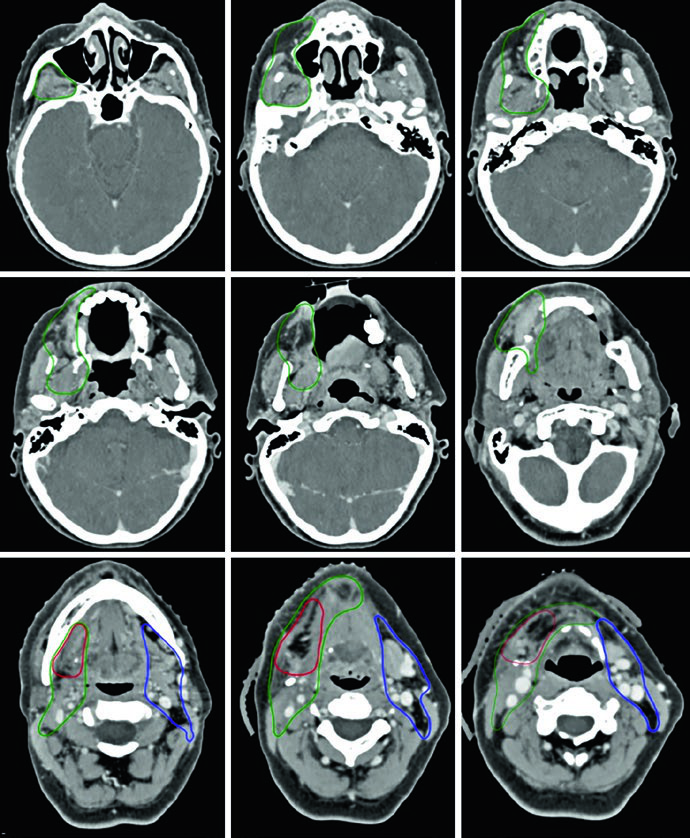
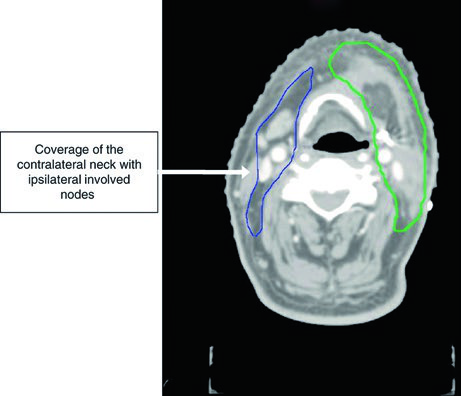
Figure 6.5 presents SCC of the buccal mucosa, T2N3b, status post-resection with right neck dissection and extranodal extension at level IB. Margins were negative but close along the deep margin. The CTV66 (red) covers the nodal region with extranodal extension.
The CTV60 includes the operative bed and the entire buccal mucosa, with ipsilateral levels I through IV. The CTV extends cranially to the buccal-gingival sulcus and infratemporal fossa at the inferior orbital rim, caudally to the buccal-gingival sulcus and submandibular gland, anteriorly to at least the lip commissure, and posteriorly to the retromolar trigone. Wide margins are necessary even for smaller primary tumors. Skin bolus is placed for adequate coverage of the high- and intermediate-risk CTVs.
The CTV54 includes contralateral levels I through III due to the extent of nodal disease in the ipsilateral neck. This case illustrates how the presence of extranodal extension significantly expands the required treatment volumes.
Clinical Case: Floor of Mouth T4aN2b
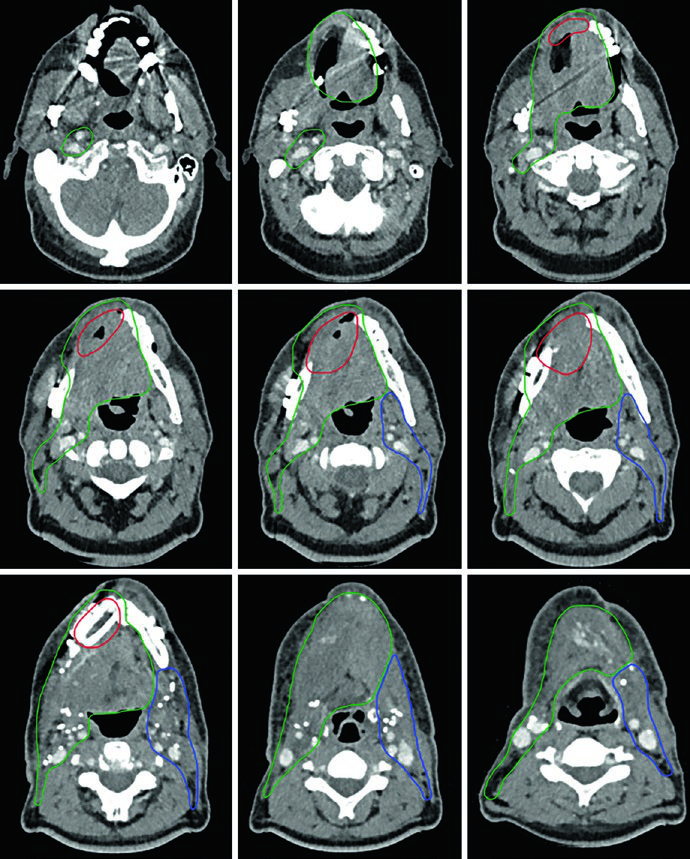
Figure 6.6 demonstrates SCC of the floor of mouth, T4aN2b, with mandibular invasion, status post-right hemi-mandibulectomy and bilateral neck dissection. The CTV66 (red) encompasses the area of extensive bony invasion. The CTV60 (green) includes the entire operative bed and ipsilateral levels I through V.
The ipsilateral retrostyloid space is included in the CTV60 as a high-risk area for nodal metastasis, especially with level II involvement. The CTV60 is also extended to include the entire floor of mouth complex. The CTV54 (blue) covers contralateral levels I through IV.
This case demonstrates how extensive mandibular invasion requires aggressive high-risk region delineation, while bilateral nodal disease justifies broad cervical coverage. In practice, floor of mouth treatment frequently requires IMRT with careful planning to limit dose to the remaining mandible, salivary glands, and airway.
Practical Planning Considerations
Several practical aspects deserve attention when planning radiation for the oral cavity. The choice between definitive and postoperative treatment depends on factors such as resectability, functional status, and institutional preference. At most centers, resectable T1-T2 tumors are managed surgically with adjuvant radiation when indicated, while locally advanced tumors (T3-T4) frequently require combined modality approaches.
The use of tissue-equivalent bolus warrants special attention. In cases with extranodal extension, surgical scars in at-risk areas, and superficial soft tissue involvement, bolus is essential to ensure prescribed dose reaches the skin surface. Without it, the build-up effect of photon beams can underdose the skin and subcutaneous tissue — precisely the regions where local recurrence is most feared.
Radiopaque wire marking of scars and drains during simulation is a simple but frequently overlooked step. This marking allows the planner to accurately identify areas of surgical manipulation on the planning CT, facilitating appropriate expansion of postoperative volumes. In clinical experience, cases where this marking was omitted resulted in uncertainty regarding the exact location of the operative bed.
The retrostyloid space and retropharyngeal lymph nodes represent distinct decisions. The ipsilateral retrostyloid space should be included in intermediate- to high-risk volumes when level II is involved, as it functions as a natural extension of the upper cervical chain. Retropharyngeal nodes, however, are generally at low risk in the oral cavity and do not require routine coverage — unlike in nasopharyngeal or oropharyngeal primaries.
Level VI inclusion is a recommendation gaining increasing traction. This level, located in the central compartment of the neck, represents a real drainage site for oral tongue tumors, and its omission in node-positive patients may leave a significant gap in coverage.
For tumors of the hard palate, the approach differs fundamentally. Most hard palate malignancies are of salivary gland origin — adenoid cystic carcinoma being the most common — rather than squamous cell carcinoma. These tumors have a strong propensity for perineural invasion, particularly along branches of the trigeminal nerve. Coverage of the nerve track toward the base of skull may be more important than cervical nodal coverage, since the rate of lymphatic spread is notably lower than in other oral cavity subsites. The treating physician may reasonably choose to omit neck treatment altogether in well-selected cases.
For further insight into target volumes in neighboring head and neck sites, see our articles on larynx cancer, hypopharyngeal carcinoma, and sinonasal tumors.


