

Thyroid cancer target delineation begins with the right imaging, stable immobilization, and exact GTV, CTV, and PTV contours on every slice of the planning CT. In this chapter, gross disease or a tumor bed with positive margins is treated to 66-70 Gy, while at-risk subclinical regions receive 54-63 Gy.
The first planning decision can affect the entire downstream pathway: iodinated contrast on CT should be avoided if the patient may still need radioactive iodine, because uptake can be impaired for as long as 6 months. MRI and ultrasound are useful when the key question is lymphadenopathy or extrathyroidal extension, and FDG-PET becomes especially relevant in poorly differentiated or anaplastic disease because those tumors may be FDG-avid.
The simulation CT is not just for setup documentation. It guides GTV contouring, particularly for lymph nodes, so any decision to use iodinated contrast needs explicit justification before it is given. For the broader series context, see our complete guide on target volume delineation and field setup.
In This Article
Thyroid Cancer Target Delineation: General Principles
Physical examination alone is not enough. The chapter’s workflow starts with a careful exam, adds staging imaging, and ends with a simulation that keeps the head, neck, and shoulders reproducible from fraction to fraction, because the treatment margin is small and often shared with the spinal cord, larynx, esophagus, and lung.
A thermoplastic mask that immobilizes the head, neck, and shoulders is preferred over head-and-neck-only immobilization. The head should be slightly extended to lower oral cavity dose. That detail matters when the target runs through the central compartment and forces the plan to work around laryngeal and tracheoesophageal structures.
The fractionation guidance is equally concrete: 30-35 fractions, delivered either as an all-in-one dose-painted IMRT plan or as an initial IMRT course followed by a boost. The recommended daily fraction size for CTVs is 1.8-2 Gy. The structure is deliberate: high dose for gross disease or a bed with clearly concerning margins, intermediate dose for meaningful subclinical risk, and 54 Gy when nodal regions are considered uninvolved but still worth elective treatment.
The chapter also makes clear that GTV and CTV must be delineated on every planning CT slice. That is not treated as a clerical step. The quality of thyroid IMRT depends on selecting the gross-disease CTV and the subclinical CTV correctly, because that is where the difference lies between a plan that is tight and a plan that is simply incomplete.
Target Volumes for Gross Disease
For gross disease, the logic is straightforward: everything visible on examination and imaging belongs in GTV66-70, and cervical lymph nodes become gross disease when they are at least 1 cm or contain a necrotic center. Expansion to CTV66-70 and PTV66-70 is allowed, but the chapter trims those margins when the spinal cord is immediately adjacent.
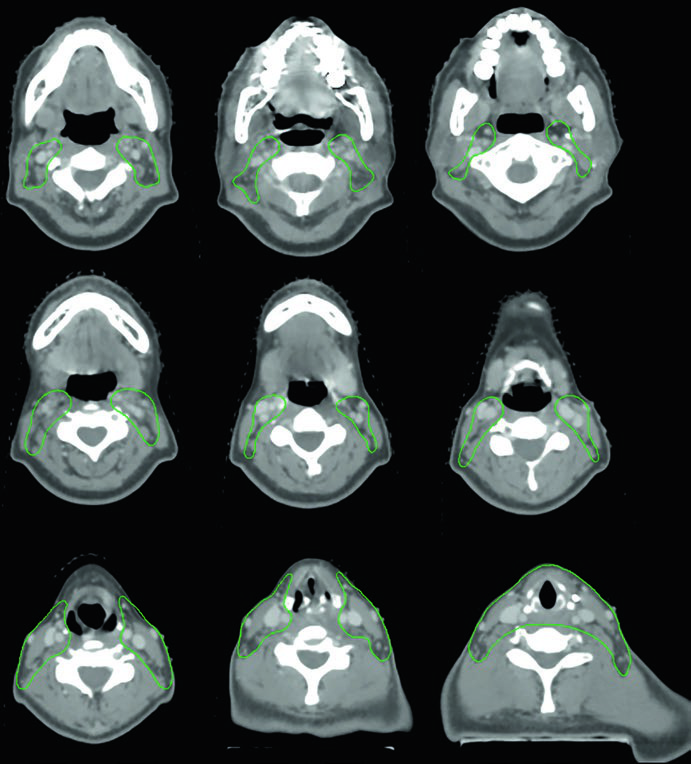
Table 9.1: suggested target volumes for gross disease
The table below captures the chapter’s high-dose logic. It shows when GTV can remain unchanged, when uncertainty justifies an added margin, and when a suspicious small node can reasonably be treated to 66 Gy rather than 70 Gy.
| Target volume | Definition and description |
|---|---|
| GTV66-70 | Primary: all gross disease on physical examination and imaging. Neck nodes: all nodes ≥1 cm or with a necrotic center. |
| CTV66-70 | Usually the same as GTV66-70. If a margin is needed because of uncertainty in gross disease extent, add 3-5 mm so that GTV66-70 + 3-5 mm = CTV66-70. If the GTV is adjacent to the spinal cord, a 1-mm margin is acceptable because spinal cord protection is required. For suspicious nodes that are small (<1 cm), a lower dose of 66 Gy, that is CTV66, can be considered. |
| PTV66-70 | CTV66-70 + 3-5 mm, depending on variability in daily patient positioning. If the CTV is adjacent to the spinal cord, a 1-mm margin is acceptable. |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 9.1)
The footnote matters as much as the table itself. The suggested dose for gross disease is 70 Gy, but 66 Gy may be chosen when the main concern is toxicity to the brachial plexus, larynx, spinal cord, lung, or esophagus. In postoperative cases with gross resection but major concern for residual disease because of positive margins, the tumor bed or the region of concern may be treated to 66 Gy.
That makes the postoperative decision cleaner than it first appears. The chapter does not recommend enlarging the high-dose region by reflex. It asks whether there is real concern for residual disease and how close the plan will run to critical normal structures.
Target Volumes for At-Risk Subclinical Disease
The at-risk subclinical volume is not just a halo around the high-dose region. In thyroid cancer, the chapter directs this CTV toward the tracheoesophageal groove, the postoperative tumor bed, and the cervical nodal pathways that actually change regional recurrence risk.
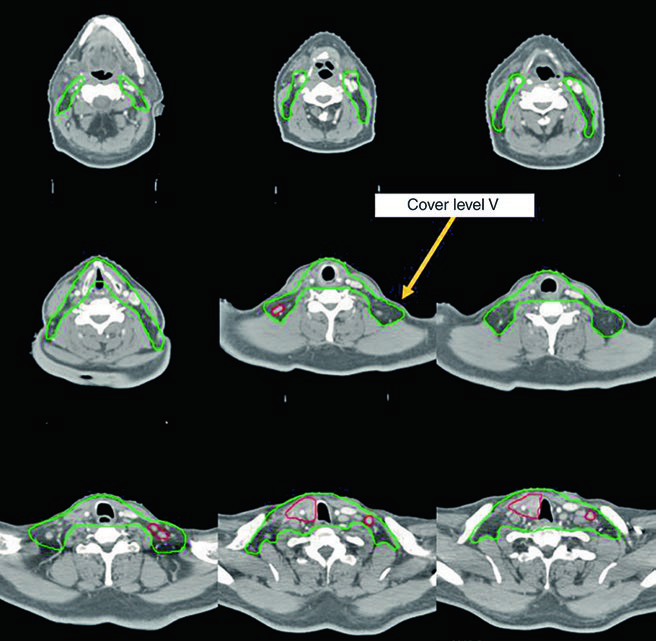
Table 9.2: suggested target volumes for the at-risk subclinical region
Table 9.2 is the chapter’s most practical guide for deciding what belongs in 60-63 Gy and what can remain at 54 Gy. It shows when to cover both lateral necks, when to extend the field to the carina, and which structures may be left out if they are not immediately adjacent to tumor or tumor bed.
| Target volume | Definition and description |
|---|---|
| CTV54-63 | Primary: should include the tracheoesophageal groove and a >5 mm margin around any CTV66-70. In the postoperative setting, it should encompass the tumor bed and the tracheoesophageal groove on the involved side or sides. If a tracheostomy was performed, it should also encompass the tracheostomy stoma to the skin surface. Ideally, the upper larynx (vocal cords/arytenoid cartilage and above) and posterior esophagus should be excluded if they are not adjacent to tumor or tumor bed. Lateral neck regions: include bilateral nodal levels II-VII. However, the lateral necks may be omitted when the central compartment and upper mediastinum are treated down to the level of the carina. Level I and retropharyngeal nodes are generally omitted unless they are at risk. |
| PTV54-63 | CTV54-63 + 3-5 mm, depending on variability in daily patient positioning. If the CTV is adjacent to the spinal cord, a 1-mm margin is acceptable. |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 9.2)
The footnote compresses the dose logic into one line: 60-63 Gy for at-risk subclinical disease, with the option to treat uninvolved nodal regions judged to be low risk to 54 Gy at the treating physician’s discretion. That is why the chapter alternates between broad bilateral neck coverage and plans that stay focused on the central compartment and descend into the superior mediastinum.
Two choices recur throughout the text. One is to treat the tracheoesophageal groove almost as a signature part of the CTV, especially when the problem sits near the trachea, esophagus, or a postoperative margin. The other is to exclude the upper larynx and posterior esophagus when they are not touching the target. That is not cosmetic sparing. It is an attempt to reduce unnecessary dose without breaking the anatomic logic of the plan.
What the Chapter’s Cases Show in Practice
The case figures repeat the same lesson under different conditions: the final target is not decided by histology alone. The decisive factors are resectability, where recurrence sits, whether margins remain positive, how far the plan must descend into the mediastinum, and whether the dominant risk lives in the central compartment or in the lateral neck.
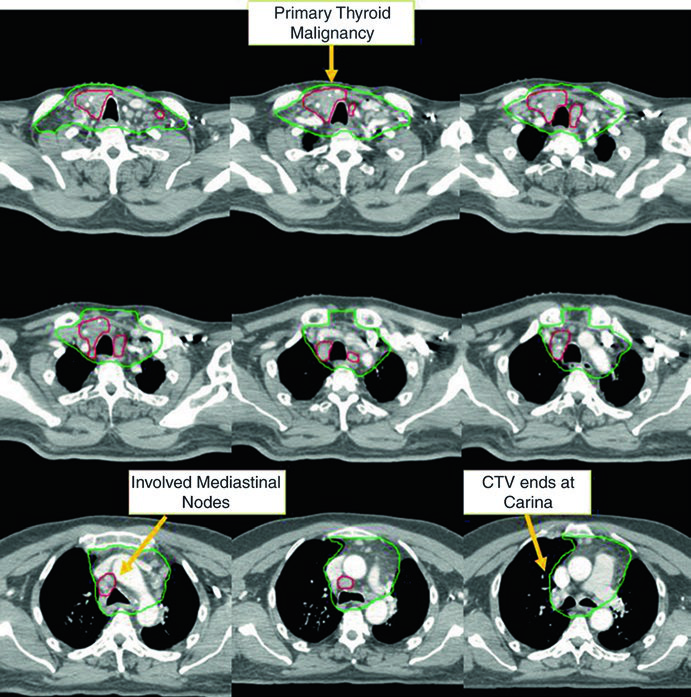
Fig. 9.1: unresectable local recurrence with mediastinal lymph nodes
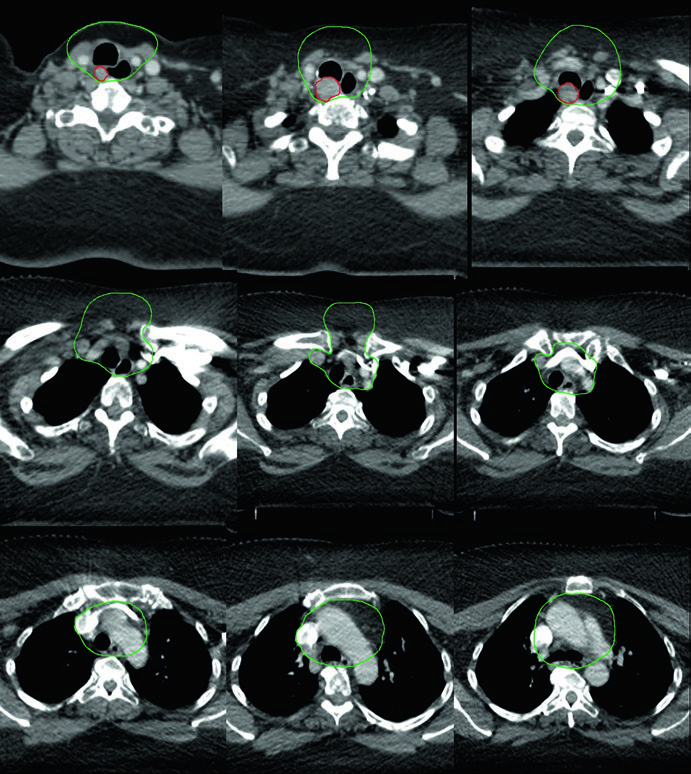
The first vignette is a 58-year-old man with metastatic papillary thyroid carcinoma who had already undergone multiple surgical resections before presenting with unresectable local recurrence and multiple mediastinal lymph nodes. He received definitive chemoradiotherapy to prevent local progression. The chapter labels CTV70 Gy in red and CTV60 Gy in green, emphasizing that the displayed images are only representative slices.
This case helps explain why the chapter allows omission of the lateral neck in selected situations, provided the plan covers the central compartment and continues into the superior mediastinum. Here the danger is not evenly distributed across the neck. It stays concentrated around the tracheoesophageal pathway and the visible mediastinal nodes.
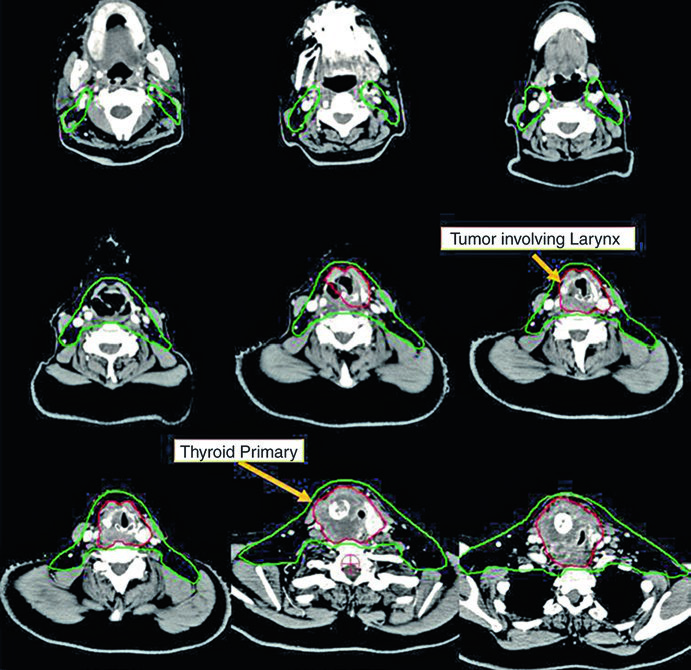
Fig. 9.2: unresectable anaplastic carcinoma invading larynx, trachea, and esophagus
The second patient, a 73-year-old woman, had unresectable anaplastic thyroid carcinoma invading the larynx, trachea, and esophagus. Treatment was definitive chemoradiotherapy with concurrent doxorubicin, again to prevent local progression. The caption adds an important planning nuance: the manubrium is not routinely included in the at-risk volume, but it was covered here because of aggressive bulky anterior neck disease.
When disease reaches the larynx, it is useful to compare that anatomy with our dedicated larynx cancer guide. In this chapter, however, the planning rule remains thyroid-specific: the volume is pulled by the direct local invasion and by the risk of progression along contiguous structures.
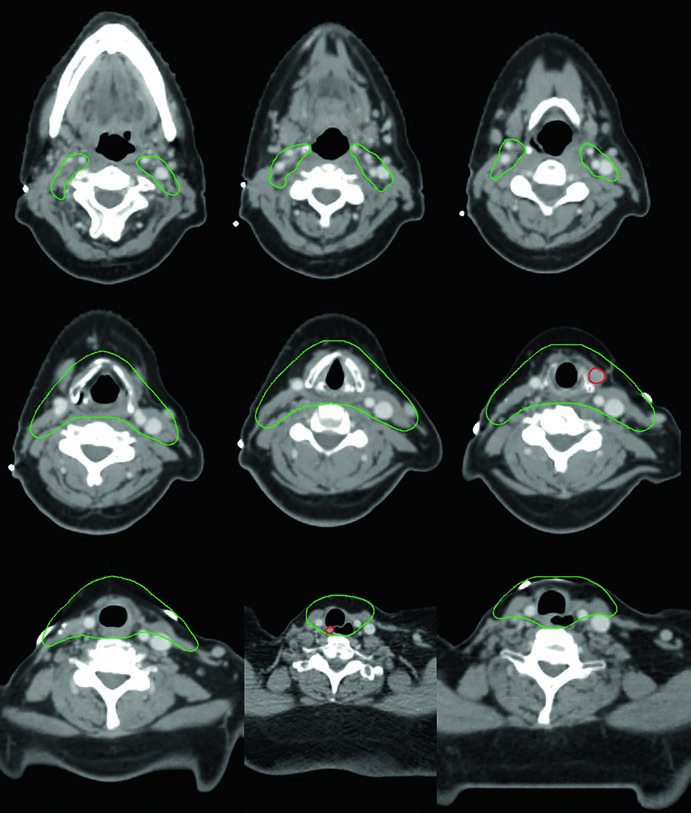
Fig. 9.3: postoperative disease with extrathyroid extension and positive margins
The third vignette describes a 50-year-old woman with anaplastic thyroid carcinoma after resection, with extrathyroid extension and positive margins but no involved lymph nodes. She received postoperative chemoradiation. The chapter explicitly notes that CTV70 Gy includes the tumor bed and the surgical clips. That is the practical expression of Table 9.1: a postoperative region can enter the high-dose volume when residual disease remains a real concern.
Fig. 9.4: multifocal recurrence after three prior surgeries
Another patient, a 61-year-old woman with a metastatic tall cell variant of papillary thyroid cancer, had three previous operations before presenting with multifocal recurrence. She was treated with definitive chemoradiation. In this figure the book uses GTV70 Gy in red and CTV60 Gy in green, reinforcing the distinction between discrete gross disease and the surrounding at-risk region.
This is the case that best illustrates why the instruction to contour GTV and CTV on every CT slice is not optional. The recurrence pattern is multifocal rather than linear, so the high-dose target has to remain faithful to the imaging and the clinical exam rather than to a broad geometric expansion.
Fig. 9.5: paratracheal recurrence with a central-compartment focus
The fifth vignette does not have an extracted image in the prompt, but the caption is still informative. It describes a 69-year-old woman with poorly differentiated thyroid cancer of follicular phenotype, adherent to the trachea and esophagus, previously treated with resection and radioactive iodine, who recurred with a right paratracheal mass invading the trachea, then underwent resection and neck dissection before adjuvant chemoradiation. Here the CTV60 Gy is shown in green, and the lateral neck was omitted because the highest recurrence risk lay in the central compartment.
Postoperative Decisions and Field Arrangement
Postoperative planning in this chapter is not automatic field expansion. The key questions are where the tumor bed sits, whether the tracheoesophageal groove is at risk, and whether a tracheostomy was performed. From there, CTV54-63 may include the tumor bed, the involved tracheoesophageal groove, and the stoma to the skin, while CTV66-70 stays reserved for positive margins or regions with credible concern for residual disease.
Field arrangement follows the same logic. Bilateral lateral neck coverage through levels II-VII is the broad default, but it is not the only acceptable plan. When the main threat lies in the central compartment and superior mediastinum, the chapter explicitly allows omission of the lateral neck and extension inferiorly to the carina. The deliberate exclusion of level I and the retropharyngeal nodes, unless they are specifically at risk, shows that this is not a chapter about indiscriminate coverage.
Two final constraints run through the entire discussion: PTV margins of 3-5 mm based on daily setup variability, with 1 mm accepted when the spinal cord defines the limit; and active exclusion of the upper larynx and posterior esophagus when those structures are not abutting the target. To place this thyroid chapter back into the full anatomical framework of the series, return to the complete guide.


