

This target volume delineation and field setup guide brings the clinical architecture of Target Volume Delineation and Field Setup into one page. The book is built for residents, radiation oncologists, medical physicists, dosimetrists, and therapists who need to turn current techniques into safe treatment planning, with explicit attention to IMRT, SBRT, and day-to-day workflow.
The opening pages make that purpose explicit: the series exists to guide contouring, recommend treatment approaches, and show when to apply different technologies without losing planning safety. In routine practice, that logic also connects well with our overview of TG-263 structure standardization, our guide to DICOM viewers for radiotherapy review, and our discussion of Monte Carlo-based dose calculation.
The material below follows the shape of the book itself: head and neck, breast and thorax, upper abdomen, pelvis, gynecology, central nervous system, lymphoma, and sarcoma. Instead of turning that into a loose list, the goal here is to show how each chapter frames the clinical problem, which planning steps appear on the opening page, and where to move next when a dedicated article is needed.
General Principles of Planning and Target Delineation
The series presentation insists on a point that still matters: contouring is not an appendix to the plan. It decides when to use the available technologies and how to perform safe treatment planning. That is why, even as the disease site changes from nasopharynx to pancreas or from lymphoma to brain metastases, the book keeps returning to the same operational structure: anatomy, relevant diagnostic workup, simulation, daily localization, organs at risk, and dose evaluation.
That pattern repeats across the volume. Some chapters start from anatomy and patterns of spread, others from imaging, technique selection, or competing treatment decisions, but the methodological backbone is consistent.
Head and Neck Chapters at a Glance
The first major block of the book covers head and neck disease with repeated emphasis on anatomy, spread, simulation, and treatment planning.
| Chapter | Disease site | Opening focus |
|---|---|---|
| 1 | Nasopharyngeal carcinoma | General principles of planning and target delineation |
| 2 | Oropharyngeal carcinoma | Introduction; anatomy and patterns of spread; workup; simulation; IMRT schemes |
| 3 | SBRT for head and neck cancer | Clinical selection for elderly and frail patients |
| 4 | Larynx cancer | Subsites, spread patterns, workup, localization, treatment planning |
| 5 | Hypopharyngeal carcinoma | Anatomy, workup, simulation, target delineation |
| 6 | Oral cavity cancers | General planning and target delineation |
| 7 | Nasal cavity and paranasal sinus tumors | Anatomy, workup, simulation, treatment planning |
| 8 | Major salivary glands | General planning and target delineation |
| 9 | Thyroid cancer | General planning and target delineation |
| 10 | Unknown primary in head and neck | General planning and target delineation |
Source: Target Volume Delineation and Field Setup, 2nd Edition (contents pages and chapter opening pages).
Nasopharyngeal Carcinoma
The nasopharynx chapter opens the book with a direct focus on general principles of planning and target delineation. That editorial choice sets the tone for the whole volume: before any disease-specific nuance, the target has to be defined methodically. To follow that logic in full, read the dedicated article on nasopharyngeal carcinoma.
Oropharyngeal Carcinoma
For the oropharynx, the text starts with the anatomy that matters clinically: tumors of the tonsils, base of tongue, soft palate, and posterior pharyngeal wall. The opening also highlights the frequent HPV association, the contrast with tobacco- and alcohol-related disease, and the chapter sequence that follows: patterns of spread, workup, simulation, daily localization, IMRT fractionation schemes, and suggested target volumes. For the full workflow, see the detailed oropharyngeal carcinoma article.
SBRT for Cancers of the Head and Neck
The SBRT chapter opens from a practical clinical position, not from technology alone. It describes advanced head and neck cancer as a disease often seen in older patients, with poor outcomes despite aggressive multimodality therapy. Fit patients may still choose radical high-dose radiation, while frail patients require a shorter-course discussion shaped by preference, tumor factors, life expectancy, and tolerance of aggressive treatment. The dedicated article expands that decision framework for head and neck SBRT.
Larynx Cancer
The larynx chapter organizes anatomy into three subsites: supraglottis, glottis, and subglottis. For the supraglottis, the book names the ventricles, false vocal cords, arytenoids, aryepiglottic folds, and epiglottis, then adds one very practical planning point: bilateral elective nodal irradiation is warranted for all supraglottic larynx cases. From there the chapter moves into workup, daily localization, and treatment planning. For the full discussion, see the detailed larynx cancer article.
Hypopharyngeal Carcinoma
For hypopharynx, the anatomy is anchored with practical landmarks: the region extends between the oropharynx and the cervical esophagus, from the top of the hyoid bone at about C4 to the bottom of the cricoid cartilage at about C6. The chapter stresses three subsites, a tendency for submucosal spread, and easy extension across neighboring structures, with direct consequences for speech and swallowing. To work through that logic in depth, read the dedicated hypopharyngeal carcinoma article.
Oral Cavity Cancers
The oral cavity chapter starts with the workup that supports every contour: comprehensive oral examination, biopsy, and imaging for staging and planning. CT is positioned as the key tool for local extent, cervical nodes, and invasion of the mandible, maxilla, and pterygopalatine fossa; MRI becomes the better study for soft-tissue extension and perineural spread; PET helps with regional nodal involvement and distant disease. The dedicated article goes deeper into oral cavity target delineation.
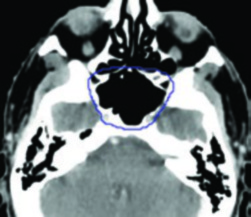
Nasal Cavity and Paranasal Sinus Tumors
For sinonasal tumors, the book makes one thing clear immediately: this is not a single biological problem. The opening page lists very different histologies, including squamous cell carcinoma, minor salivary gland adenocarcinoma, adenoid cystic carcinoma, esthesioneuroblastoma, and sinonasal undifferentiated carcinoma. Because the nasal cavity and paranasal sinuses communicate through multiple ostia and thin septa, local extension into adjacent spaces becomes central to planning. For the full chapter, open the detailed article on nasal cavity and paranasal sinus tumors.
Major Salivary Glands
The major salivary gland chapter defines the imaging package early: contrast-enhanced CT or MRI from skull base to clavicles. MRI receives special emphasis because it visualizes the tumor more clearly, helps define margins, shows deep extent, and clarifies infiltration patterns, especially on T1-weighted sequences. To review that approach carefully, read the detailed article on major salivary gland target delineation.
Thyroid Cancer
In thyroid cancer, the chapter draws one practical boundary very clearly: iodinated contrast on CT should be avoided when the patient may still need radioactive iodine, because uptake can be impaired for up to 6 months. The text also points to MRI and ultrasound for nodal assessment and extrathyroidal extension, and reminds the reader that poorly differentiated or anaplastic disease may be FDG-avid. For the full volume-delineation discussion, see the detailed thyroid cancer article.
Unknown Primary in the Head and Neck
For unknown primary disease, the book refuses to shortcut the diagnostic stage. Before accepting an unknown origin, it asks for a careful physical examination with cranial nerve assessment, fiberoptic evaluation of the nasopharynx, oropharynx, larynx, and hypopharynx, plus high-resolution contrast CT and a detailed skin and scalp examination. To review that entire workup path, see the dedicated article on unknown primary head and neck cancer.
Early Breast Cancer
For early breast cancer, the chapter places 3D conformal radiotherapy with appropriate compensation, such as field-in-field and mixed energies, as the standard adjuvant technique. It also states that the highest level of evidence supports hypofractionated whole-breast irradiation, reviews tumor-bed boost logic, and notes that APBI can be acceptable in selected low-risk patients with unifocal disease. The full discussion appears in our dedicated early breast cancer article.
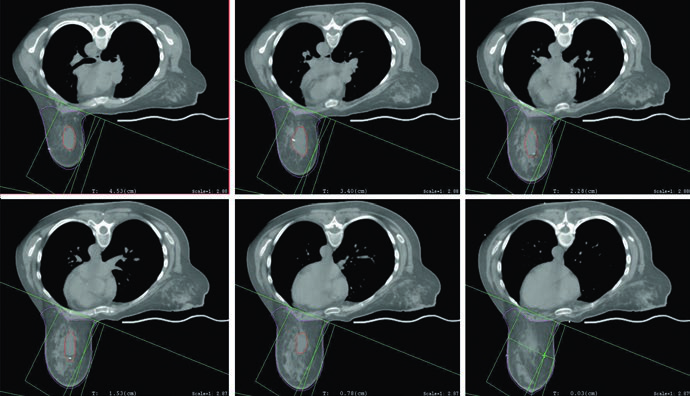
Regional Lymph Node Irradiation for Breast Cancer
The regional nodal breast chapter is highly operational. CT simulation is done with both arms above the head on a breast board, IV contrast is optional, the breast borders and lumpectomy scar may be wired, and scanning should extend from the cricoid to 5 cm below the clinically marked inferior field edge while including both lungs. From there the chapter moves into unreconstructed and reconstructed chest wall cases and conformal planning. For the full workflow, read the article on regional nodal irradiation in breast cancer.
Breast, Thoracic, and Upper Abdominal Chapters
This group of chapters pulls technique, imaging, and motion management together in a very practical way.
| Chapter | Disease site | Opening focus |
|---|---|---|
| 11 | Early breast cancer | General planning and target delineation |
| 12 | Regional nodal irradiation in breast cancer | Nodal target delineation and chest wall scenarios |
| 13 | Lung cancer | Planning, motion management, nodal levels |
| 14 | Esophageal cancer | Planning and target delineation |
| 15 | Gastric cancer | Anatomy, workup, postoperative CTV scenarios |
| 16 | Pancreatic cancer | General target delineation and planning |
| 17 | Hepatocellular carcinoma | General planning and target delineation |
Source: Target Volume Delineation and Field Setup, 2nd Edition (contents pages and chapter opening pages).
Lung Cancer
In lung cancer, the book is explicit that CT-based planning and respiratory motion management are standard in both NSCLC and SCLC. 3D-CRT, IMRT, and SBRT use multiple beam angles and change dose conformality, so accurate delineation of targets, normal structures, and organs at risk cannot be separated from DVH review and from understanding the mediastinal nodal levels at risk. The dedicated article goes deeper into lung cancer target delineation.
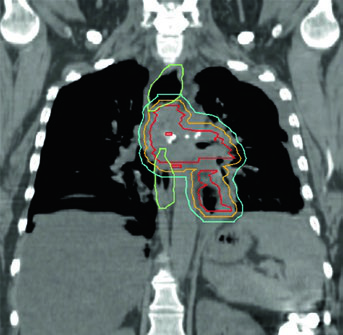
Esophageal Cancer
For esophageal cancer, the central idea remains the same: CT-based planning with conformal techniques is standard. Both IMRT and 3D-CRT require accurate target volumes, clear organ-at-risk contours, and dose-volume review, but the chapter makes one extra point that matters: the esophagus spans the neck, mediastinum, and abdomen, so planning depends on a broad anatomic read of the brachial plexus, lungs, heart, spinal cord, and normal esophagus. For the complete discussion, see the detailed esophageal cancer article.
Gastric Cancer
The gastric chapter combines anatomy and postoperative scenarios in a useful way. It reminds the reader that the stomach begins at the gastro-esophageal junction and ends at the pylorus, describes the greater and lesser curvatures, divides the organ into cardia, fundus, body, and antrum, and then moves into clinical target volumes for postoperative cases involving the cardia, body, and antrum or pylorus. To review that sequence carefully, open the detailed gastric cancer article.
Pancreatic Cancer
The pancreas chapter moves into technique immediately. IMRT is presented as an increasingly standard approach in neoadjuvant, adjuvant, and definitive settings; 3D-CRT still has a role for palliation and selected neoadjuvant cases; ablative treatment requires SBRT or image-guided techniques. The chapter also gives a concrete contrast-simulation protocol: 150 cc at 5 cc/s, with late arterial imaging at 35 s and portal venous imaging at 90 s, especially critical when dose exceeds 50 Gy in EQD2. The dedicated article covers pancreatic planning in full detail.
Hepatocellular Carcinoma
For primary liver disease, the opening page itself shows the authors’ priority: general principles of planning and target delineation, followed by further reading. That structure is a reminder that in liver radiotherapy the logic of the volume comes before any isolated prescription number. To follow that reasoning in the dedicated text, open the article on hepatocellular carcinoma.
Rectal Cancer
The rectal cancer chapter is organized as a practical workflow: diagnostic workup relevant to delineation, simulation and daily localization, target-volume definition, and plan assessment. That sequence matters because in pelvic planning the error rarely starts at the last step; it usually starts earlier, in the way the case is prepared. To follow the chapter in detail, see the dedicated rectal cancer article.
Anal Cancer
For anal cancer, the book gives an anatomic anchor that is both simple and useful: the anal canal is about 4 cm long, extending from the proximal anorectal ring to the distal anal verge. From that point the chapter structures anatomy, spread patterns, workup, simulation, delineation, and plan assessment. To see how that becomes a treatable volume, read the detailed anal cancer article.
Postoperative Gynecologic Therapy
In the postoperative gynecologic setting, the introduction is direct: IMRT has become the treatment of choice for adjuvant radiotherapy in cervical and endometrial malignancies. The chapter also cites a phase III randomized trial showing significant reductions in acute GI and GU toxicity, better quality of life, and less irradiated bone marrow when compared with 3D conformal treatment. For the full version, see the dedicated postoperative gynecologic radiotherapy article.
Definitive Gynecologic Therapy
For definitive gynecologic therapy, the book shows a field in transition. IMRT is presented as an increasingly common strategy, even without large randomized trials, supported by phase II studies and controlled series suggesting effectiveness with less toxicity. The chapter walks through staging, CT simulation, target delineation, organs at risk, plan assessment, image-guided delivery, and separate cervical, vaginal, and endometrial scenarios. To go deeper, read the dedicated definitive gynecologic radiotherapy article.
Image-Guided Brachytherapy
Image-guided brachytherapy earns its own chapter because the workflow does not fit into a short note. The contents page already shows the breadth of the subject: general principles, cervical cancer with applicator choice, implant evaluation, delineation, and treatment planning, followed by endometrial, vaginal, and vulvar scenarios. To review that organization in full, open the detailed image-guided brachytherapy article.
Vulvar Cancer
The vulvar chapter is direct in calling this one of the most complex sites in radiation therapy. Large treatment volumes and high morbidity rates, especially with intensive chemoradiation for advanced disease, explain the emphasis on IMRT, simulation, image registration, target delineation, prescription, organs at risk, and image-guided treatment. For the full reading, see the dedicated vulvar cancer article.
Advanced Gynecologic Technologies
In the advanced technologies chapter, the authors are clear about the problem they are trying to solve: outcomes remain suboptimal in locoregionally advanced gynecologic malignancies, and treatment toxicity can limit delivery. That is why the chapter is built around image guidance, bone-marrow-sparing IMRT, adaptive replanning, proton therapy, and SBRT. To follow that technical agenda in greater detail, read the dedicated article on advanced gynecologic technologies.
Prostate Adenocarcinoma
For prostate adenocarcinoma, the chapter is concise: IMRT is the standard technique for external beam treatment in both definitive and postoperative settings, either alone or combined with brachytherapy. Different fractionation schemes exist, but all of them rely on the same foundation: accurate target delineation and image-guided treatment delivery. The dedicated text details those choices for prostate adenocarcinoma.
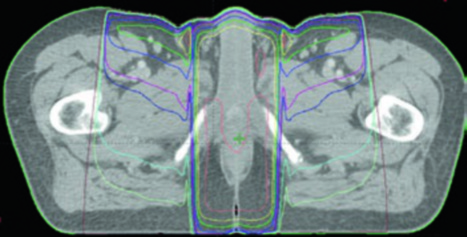
Bladder Cancer
For bladder cancer, organ preservation with trimodality therapy is presented as a standard definitive option for node-negative muscle-invasive disease, beginning with maximal and ideally complete TURBT followed by concurrent chemoradiotherapy. The chapter also separates the node-positive scenario, recalls the historical role of 3D conformal treatment in RTOG/NRG protocols, and incorporates the more recent acceptance of IMRT, along with MSKCC guidelines. For the complete content, see the article on bladder cancer target delineation.
Testicular Seminoma
In seminoma, almost everything starts with radical inguinal orchiectomy. The chapter makes it clear that postoperative management depends on histologic subtype and disease extent, and that radiation is generally reserved for pure seminoma while rarely used for non-seminomatous germ cell tumors. Before any decision, the workup includes history, physical examination, AFP, beta-hCG, LDH, chemistry panel, testicular ultrasound, and chest radiography. To review that pathway, open the dedicated testicular seminoma article.
Pelvic, Gynecologic, and Genitourinary Chapters
The pelvic section presents a clear sequence from staging and setup to delineation and plan review.
| Chapter | Disease site | Opening focus |
|---|---|---|
| 18 | Rectal cancer | Workup, simulation, target delineation, plan assessment |
| 19 | Anal cancer | Anatomy, workup, simulation, treatment planning |
| 20 | Postoperative gynecologic therapy | Introduction, workup, treatment planning |
| 21 | Definitive gynecologic therapy | Staging, CT simulation, target delineation, OARs |
| 22 | Image-guided brachytherapy | Applicator choice, implant evaluation, planning |
| 23 | Vulvar cancer | General principles, simulation, image registration, OARs |
| 24 | Advanced gynecologic technologies | Image guidance, marrow-sparing IMRT, adaptive replanning |
| 25 | Prostate adenocarcinoma | General planning and target delineation |
| 26 | Bladder cancer | 3D-CRT, IMRT, simulation, MSKCC guidelines |
| 27 | Testicular seminoma | General planning and target delineation |
Source: Target Volume Delineation and Field Setup, 2nd Edition (contents pages and chapter opening pages).
Brain Metastases
For brain metastases, the opening page frames the decision that most strongly reorganizes planning: whole-brain radiation therapy or stereotactic radiosurgery. The text notes that the choice depends on number and volume of metastases plus performance status, and it summarizes a clinically important contrast: SRS better preserves neurocognitive function and quality of life, whereas WBRT improves distant and overall intracranial control. To see the full chapter structure, read the detailed brain metastases article.
Benign CNS Tumors
The benign CNS tumor chapter is broad because the disease group is broad. After general planning and delineation principles, it moves through positioning, immobilization, simulation, normal structures, and then low-grade astrocytic and oligodendroglial tumors, meningioma, vestibular and non-vestibular schwannoma, pituitary tumors, and glomus tumors or paraganglioma. To review that entire map, see the dedicated benign CNS tumors article.
Malignant CNS Tumors
For malignant CNS tumors, the chapter opens by asking for a detailed history, a focused neurologic examination, and appropriate laboratory investigations. The contents page then places the classic elements of neuro-oncology planning in order: positioning, immobilization, simulation, normal structures, and later the high-grade glioma section. The dedicated text details that planning logic for malignant CNS tumors.
Hodgkin and Non-Hodgkin Lymphoma
The lymphoma chapter stands out because it organizes field setup and tumor volume together. The authors begin with general delineation and setup principles, move into involved-site and involved-node radiation therapy, add case-based examples, and finish with contouring for inguinal-pelvic, gastric, orbital, and sinonasal presentations. To review that full pathway, see the dedicated lymphoma article.
Soft Tissue Sarcoma
In soft tissue sarcoma, the chapter is unusually specific about how spread should change the target. Anatomic location, size, depth, and pathology guide management; invasion is usually longitudinal within muscle and within the compartment of origin; suspicious edema may contain microscopic disease and should ordinarily be included; and barriers such as bone, interosseous membrane, and major fascial planes should be used in function-preserving planning. For the full chapter, open the article on soft tissue sarcoma.
Pediatric Sarcoma
The pediatric sarcoma chapter makes it clear that sarcoma in childhood is not one disease. It brings together bone tumors and soft tissue sarcomas, reminds the reader that treatment algorithms vary by histology, stage, risk group, and even geography, and then anchors the discussion with two practical markers: Ewing sarcoma is the second most common pediatric bone tumor, and rhabdomyosarcoma is the most common pediatric soft tissue sarcoma. The dedicated article expands that overview for pediatric sarcoma.
Pediatric Brain Tumors
The book closes strongly with pediatric brain tumors. The chapter separates medulloblastoma, ependymoma, and pure germinoma, and the opening section quickly notes that 3D conformal therapy, IMRT, VMAT, and proton therapy can all be used successfully. The platform changes, but the core requirement does not: careful volumetric target delineation. To follow the full chapter, see the dedicated pediatric brain tumors article.
CNS, Lymphoma, Sarcoma, and Pediatric Chapters
In the final block of the book, immobilization, platform selection, special volumes, and precise anatomy reading move to the front.
| Chapter | Disease site | Opening focus |
|---|---|---|
| 28 | Brain metastases | WBRT versus SRS; general principles for both |
| 29 | Benign CNS tumors | Planning, immobilization, simulation, normal structures |
| 30 | Malignant CNS tumors | Planning, simulation, high-grade glioma |
| 31 | Hodgkin and non-Hodgkin lymphoma | Field setup, involved-site and involved-node RT |
| 32 | Soft tissue sarcoma | General planning and target delineation |
| 33 | Pediatric sarcoma | Background, imaging, target delineation, localization |
| 34 | Pediatric brain tumors | Medulloblastoma, ependymoma, pure germinoma |
Source: Target Volume Delineation and Field Setup, 2nd Edition (contents pages and chapter opening pages).
Across the full book, one message stays stable: the value of target delineation is not limited to drawing a contour. It lies in connecting imaging, anatomy, therapeutic intent, and toxicity limits. Use this guide as the map, then move to the dedicated articles whenever a site-specific workflow is needed.


