

How the Goiânia Radiological Accident Happened
On September 13, 1987, two individuals entered an abandoned radiotherapy clinic in Goiânia, Brazil, and removed the source assembly from a teletherapy machine. They had no idea what it was — they assumed it might have some scrap value. That uninformed act triggered one of the most serious radiological accidents ever recorded, causing 4 deaths, 28 radiation burns, and the contamination of an entire urban area.

The source contained caesium-137 chloride with an activity of 50.9 TBq (1375 Ci). This salt is highly soluble and readily dispersible — properties that turned the capsule rupture into an environmental and public health disaster of unexpected proportions. For a comprehensive overview of the event and its consequences, see our complete guide to the Goiânia radiological accident.
The Setting in 1980s Goiânia
Goiânia is the capital of Goiás State on the central Brazilian plateau, a region known for its cereal farms and cattle ranches. At the time of the accident, the city had about one million residents. The climate is humid, with a mean annual temperature of 21.9°C (frequently reaching 40°C) and annual rainfall of 1700 mm.
The section of the city where the accident occurred was one of its poorer areas, with limited literacy among the population. This detail matters: it explains why residents did not recognize radiation warning symbols or connect gastrointestinal symptoms to radiation exposure. The blue glow of caesium-137 in the dark fascinated people rather than alarming them.
In terms of radiation protection infrastructure, the major centres of expertise were far away. The Institute of Radiation Protection and Dosimetry (IRD) and the Nuclear Engineering Institute (IEN) were based in Rio de Janeiro, 1,348 km from Goiânia. The Institute for Nuclear and Energy Research (IPEN) was in São Paulo, 919 km away. This geographic distance directly affected the initial response time.
The Regulatory Framework and Control Failures
Brazil’s National Nuclear Energy Commission (CNEN) was — and remains — the regulatory authority for licensing radioactive sources. CNEN’s President reported directly to the President of the Republic. The commission operated three research institutes: IPEN, IRD, and IEN.
CNEN’s licensing system required both facilities and individuals to be accredited. Health physicists and radiation protection officers needed prescribed training and competency examinations. To obtain an operating licence, an organization had to employ certified personnel, submit facility plans before construction, and provide all radiation safety documentation — procedures, local rules, instrumentation, personal monitoring, and contingency plans.
A critical gap emerges here. Once a licence was granted, periodic inspection of medical facilities fell under the Federal Ministry of Health, which in turn delegated this responsibility to State Health Secretaries. The IAEA report notes that “the extent to which this responsibility was discharged varied between States.” In practice, oversight failed.
Licence conditions were explicit: any significant change in equipment or facility status had to be reported to CNEN. Moving or disposing of sources required formal notification. These requirements existed on paper. But when the Instituto Goiano de Radioterapia abandoned its premises — taking only the cobalt-60 unit and leaving the caesium-137 machine behind — CNEN was never notified.
The Instituto Goiano de Radioterapia and Source Abandonment

The Instituto Goiano de Radioterapia (IGR) was a private radiotherapy clinic owned by a medical partnership. Its facilities included teletherapy rooms with caesium-137 and cobalt-60 equipment. The IGR followed normal licensing procedures: on June 17, 1971, CNEN approved the importation of the caesium-137 source. Shortly afterward, the equipment was installed, inspected, and became operational.
Under the operating licence terms, a physicist and a physician (one of the partners) were jointly responsible for compliance. But around the end of 1985, the IGR ceased operating from those premises. A new partnership took over different facilities. The cobalt-60 unit was moved to the new location. Ownership of the old clinic’s contents was disputed — and the caesium-137 teletherapy unit remained where it was, with no one assuming responsibility for it.
What followed was progressive abandonment. Most of the clinic and surrounding properties were demolished. But the treatment rooms — where the teletherapy equipment remained — were left standing in a derelict state, apparently used by homeless people. The IAEA report is emphatic: “nothing can deflect from the fact that the professional and moral responsibility for the security of a radioactive source must lie with the person or persons licensed as responsible for it.”
The Cesapan F-3000 Machine and Its Caesium-137 Capsule
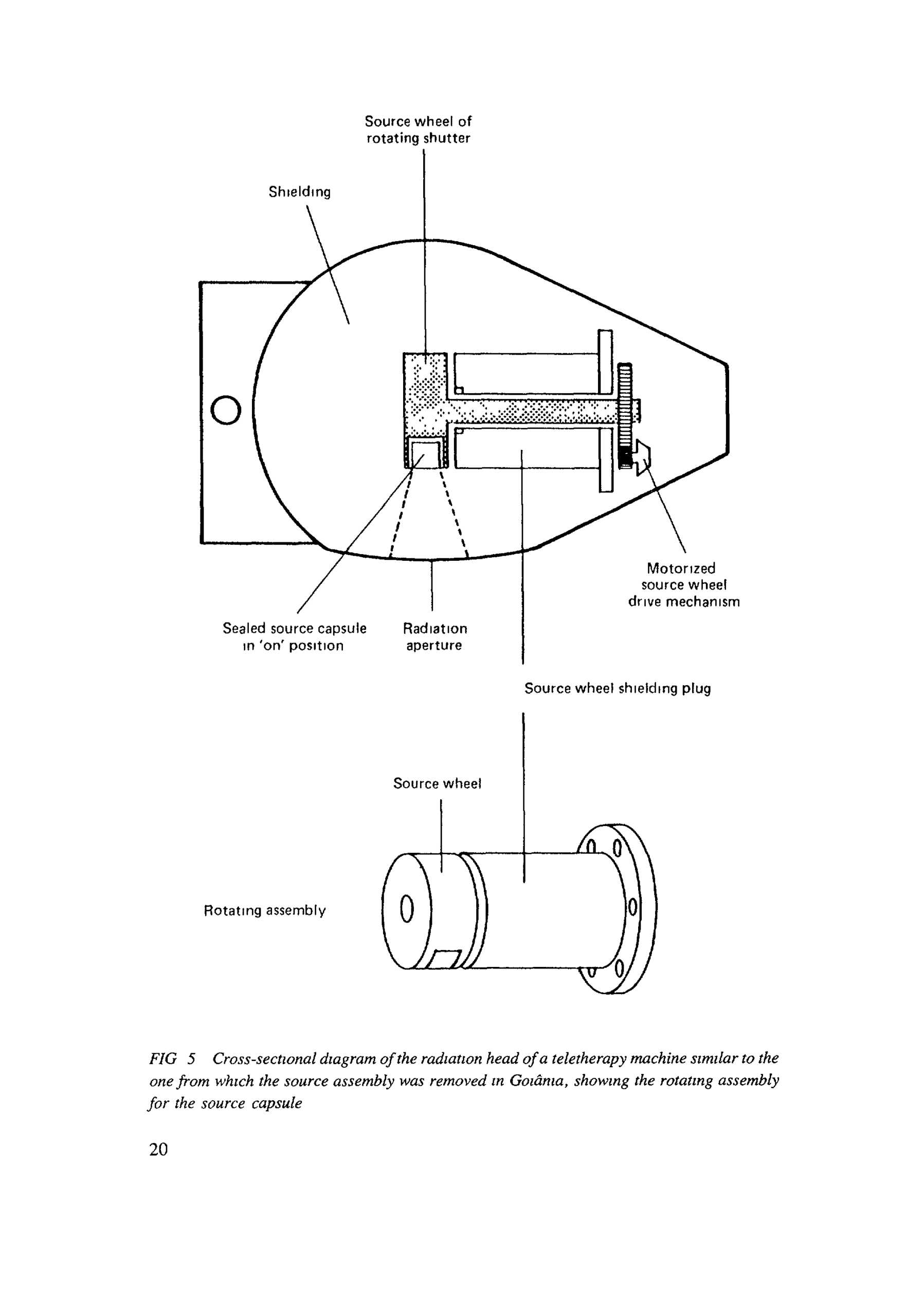
The teletherapy unit in question was a Cesapan F-3000 model, designed by Barazetti and Company of Milan in the 1950s and marketed by Generay SpA of Italy. Understanding its major components is essential to grasping how the accident unfolded.
The sealed radioactive source capsule sat within a source wheel, made of lead and stainless steel, forming the rotating shutter mechanism. To produce a radiation beam, the shutter was rotated electrically to align the source capsule with the radiation aperture. After an exposure or during a power failure, a spring-loaded device returned the shutter — and the source — to the “off” or “safe” position.
Between the rotating shutter and its electric drive mechanism was a cylindrical shielding plug. These elements — capsule, source wheel, shutter, and plug — collectively formed the “rotating assembly.” The unit was designed so this assembly could be removed from the radiation head shielding using special tools.
The key phrase is “special tools.” Removal of the rotating assembly was not supposed to be possible without proper instrumentation. In reality, however, two people with no technical training managed to extract the assembly using improvised tools. The 1950s design did not anticipate this scenario.
From Removal to Contamination: The Sequence of Events
The two individuals who entered the abandoned clinic took the source assembly home and attempted to dismantle it. In the process, the sealed capsule was ruptured. The radioactive material — caesium chloride — resembles ordinary powder but has an extraordinary property: it glows blue in the dark, a phenomenon known as radiation luminescence.
The remnants of the source assembly were sold as scrap to a junkyard owner. He noticed the material’s blue glow. Several people were fascinated by the phenomenon. Over several days, friends and relatives came to see it. Fragments the size of rice grains were distributed to multiple families.
This continued for five days. People handled the caesium chloride powder directly: they rubbed it on their skin, ate with contaminated hands, and brought it into their homes. Contamination spread to residences, furniture, utensils, and public buildings. During this period, many began showing gastrointestinal symptoms from radiation exposure — but no one made the connection.
The symptoms were not initially recognized as radiation-related. However, one of the exposed individuals connected the illnesses to the source capsule and brought the remnants to the city’s public health department. This action triggered the chain of events leading to the accident’s discovery. A local physicist was the first to assess the scale of the disaster by monitoring, and on his own initiative evacuated two areas — as detailed in our complete guide to the Goiânia accident.
The Scale of Immediate Consequences
The final numbers are staggering. In total, 112,000 people were monitored. Of these, 249 were contaminated internally or externally. Twenty people were identified as needing hospital treatment. Fourteen were admitted to the Marcílio Dias Naval Hospital in Rio de Janeiro, while the remaining six were treated at the Goiânia General Hospital.
Four casualties died within four weeks. Post-mortem examinations revealed haemorrhagic and septic complications associated with acute radiation syndrome. The best cytogenetic dose estimates for these four individuals ranged from 4.5 Gy to over 6 Gy. Two patients with similar estimated doses survived.
Environmental contamination was severe. Seven major contamination foci were identified, including the junkyards involved, with dose rates reaching up to 2 Sv/h at one metre. An aerial helicopter survey confirmed no major contamination areas had been overlooked. In all, 85 houses showed significant contamination, and 200 individuals were evacuated from 41 residences.
Decontamination generated a total waste volume of 3,500 m³ — over 275 lorry loads. This required 3,800 metal drums (200 L), 1,400 metal boxes (5 tonnes), 10 shipping containers (32 m³), and 6 sets of concrete packaging. The best estimate of radioactivity in the contamination was approximately 44 TBq (1,200 Ci), compared to the original source activity of 50.9 TBq (1,375 Ci) before the accident.
Lessons That Emerged from the Tragedy
The IAEA report emphasizes that “nothing can diminish the responsibility of the person designated as liable for the security of a radioactive source.” Sources removed from their registered location can present a major hazard. The responsible individual must ensure verification procedures and appropriate security arrangements are maintained.
Another crucial point: public recognition of the potential danger of radiation sources is an important factor in reducing the likelihood of radiological accidents. Goiânia demonstrated the need for radiation hazard marking systems that are recognizable by the general public — not just professionals.
The physical and chemical properties of radioactive sources must also be factored into manufacturing licences. Caesium chloride, being highly soluble and dispersible, enormously worsened the accident’s consequences. Sources with less hazardous properties could have limited dispersal even after capsule rupture.
The Goiânia accident did not fit the scenarios covered by existing emergency plans — which addressed either nuclear power plant accidents or smaller events involving industrial sources. The lesson is clear: radiological emergency preparedness must cover the entire range of possible accidents, not only the most probable or most easily modelled scenarios.


