

Target volume delineation in anal cancer: what drives the plan
Target volume delineation in anal cancer hinges on a thorough understanding of anal canal anatomy and its lymphatic drainage patterns. The anal canal measures roughly 4 cm in length, extending from the anorectal ring (the palpable border of the anal sphincter and puborectalis muscle) proximally to the anal verge distally. Squamous cell carcinomas arising proximal to the anal verge are managed as anal canal cancers, while those distal to the anal verge are managed as perianal skin cancers — a distinction that fundamentally changes the field design.
The dentate line (or pectinate line) marks the transition from the columnar epithelium of the proximal anal canal to the squamous epithelium distally. This embryologic junction — where endoderm meets ectoderm — is critical because it defines entirely different lymphatic drainage pathways. Proximal tumors drain preferentially to perirectal, superior hemorrhoidal, and internal iliac nodes. Distal tumors, on the other hand, drain to superficial inguinal, femoral, and external iliac nodes.
For a comprehensive overview of all anatomic sites and planning strategies, see our complete guide on target volume delineation and field setup.
Lymphatic Drainage: The Foundation of Nodal Planning
The lymphatic drainage pattern of the anal canal varies directly with the location of the primary tumor, and understanding this map is essential for deciding which elective nodal regions to cover.
| Primary Tumor Location | Draining Lymphatics |
|---|---|
| Distal anal canal, perianal skin, and anal verge | Superficial inguinal, femoral, external iliac |
| Anal canal just proximal to the dentate line | Internal pudendal, hypogastric, obturator, inferior and middle hemorrhoidal |
| Proximal anal canal and distal rectum | Perirectal, superior hemorrhoidal |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 19.1)
In practice, most anal canal tumors require coverage of both pelvic and inguinal chains. Whether the external iliac and inguinal nodes are classified as high risk or low risk depends on confirmed nodal involvement by biopsy or PET/CT.
Diagnostic Workup Relevant for Delineation
Physical examination remains irreplaceable in anal cancer staging. The evaluation should include: tumor size and location relative to the anal verge, sphincter function, invasion of adjacent structures via pelvic examination, and inguinal lymph node assessment.
Inguinal nodes that are suspicious but borderline in size deserve biopsy confirmation. Nearly 50% of clinically suspicious nodes turn out to be reactive hyperplasia — a finding that directly shifts the CTV from high risk to low risk classification.
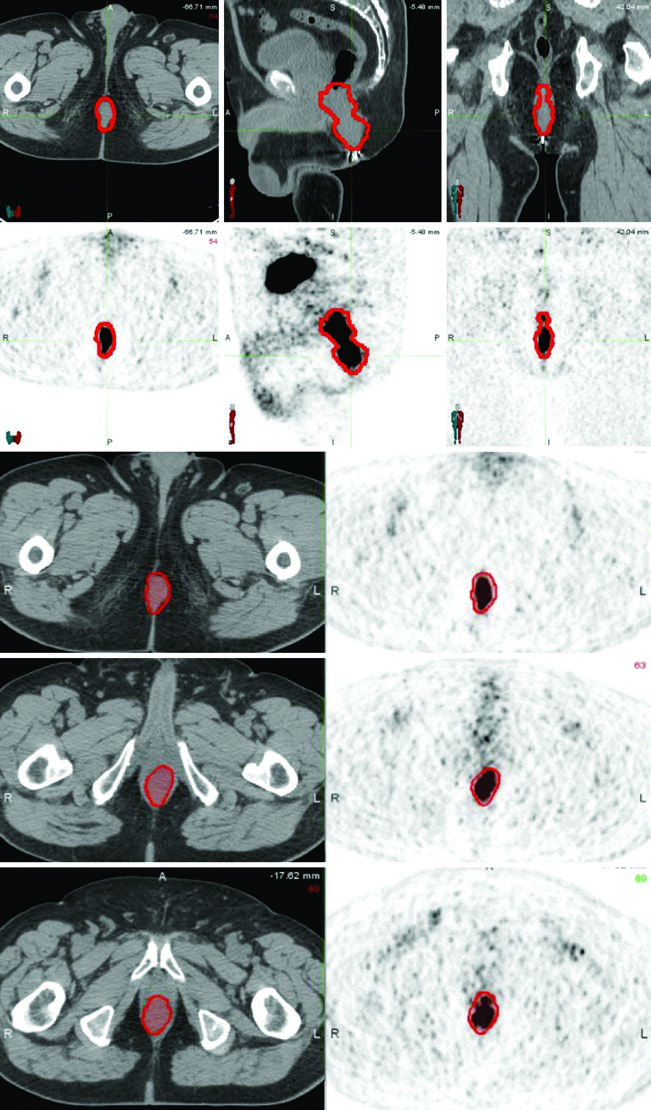
PET/CT is recommended for both staging and treatment planning to help delineate the extent of gross disease. However, areas of low uptake on PET should not supersede physical examination findings or abnormalities seen on CT or MRI. Multi-modality image integration remains the safest approach.
Simulation and Daily Localization
The patient should be simulated supine with arms on chest in a body mold. Prone positioning with a belly board can displace bowel anteriorly, but it is less reproducible and complicates bolus placement. A radiopaque marker should be placed at the anal verge.
CT simulation with intravenous contrast and slice thickness of 3 mm or less is required to delineate the pelvic blood vessels and gross tumor volume. When available, PET/CT fusion or MRI can significantly assist in target volume definition.
Bladder filling strategy matters: a full bladder may displace bowel loops out of the pelvis, while an empty bladder may be more reproducible. Daily image guidance with orthogonal kV imaging and weekly cone-beam CT scans is recommended. If there is significant variation in bladder or rectal filling, CBCT frequency should increase.
Target Volumes and Planning: From GTV to PTV
Conventional 3D conformal radiotherapy for anal canal cancers was historically complex due to the need to irradiate the pelvis and inguinal nodes simultaneously. The “thunderbird” technique was the classic approach. The RTOG 0529 trial established the feasibility of IMRT in a multi-institution setting, demonstrating lower rates of grade 2 or higher hematologic toxicity and lower rates of grade 3 or higher gastrointestinal or dermatologic toxicity compared to historical controls from RTOG 9811 using 3D conformal radiotherapy.
A key point: target delineation that is non-compliant with consensus guidelines is associated with an increased risk of disease recurrence. Contouring accuracy matters as much as the delivery technique itself.
| Target Volume | Definition and Description |
|---|---|
| GTV-P, GTV-N | GTV-P: all gross disease on physical examination and imaging. GTV-N: nodes ≥1.5 cm, PET-positive, and/or biopsy-proven. Distinguish GTV-Na (≤3 cm) from GTV-Nb (>3 cm) |
| CTV-P, CTV-N | CTV-P: GTV-P + 1.5–2.5 cm margin excluding uninvolved bone, muscle, or air. CTV-N: GTV-N + 1.0–1.5 cm excluding uninvolved bone, muscle, or air |
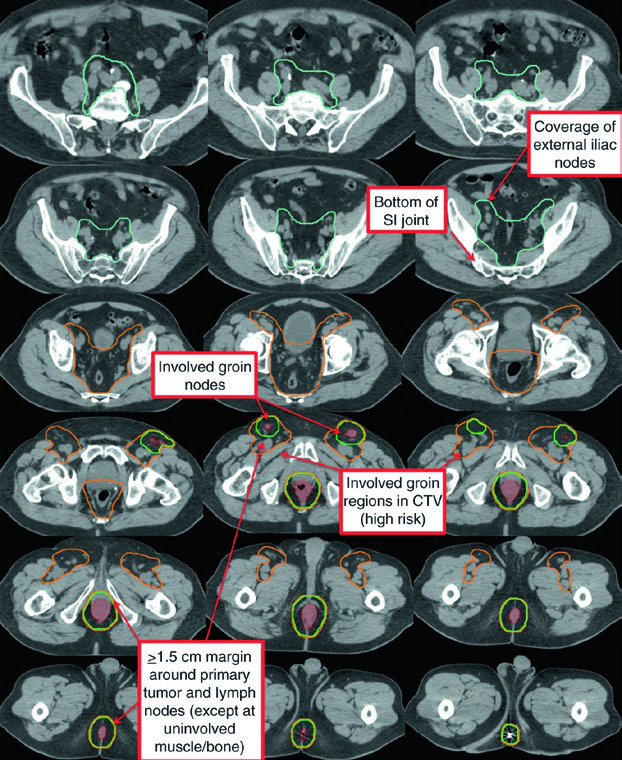
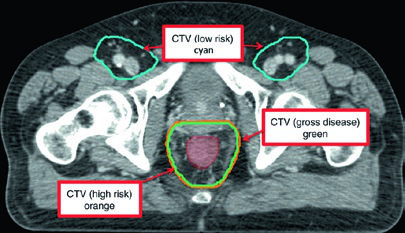
| CTV-HR (high risk) | Covers CTV-P, CTV-N, entire mesorectum, perirectal nodes, and bilateral internal iliac nodes inferior to the inferior border of the sacroiliac joint. If inguinal or external iliac nodes are involved, include these regions. 0.7 cm margin around internal iliac vessels. 1.8 cm strip between external and internal iliac vessels for obturator nodes. 1–1.5 cm anteriorly into bladder |
| CTV-LR (low risk) | Covers uninvolved internal iliac nodes superior to the sacroiliac joint inferior border, plus uninvolved external iliac and inguinal nodes. Margins: 0.7 cm around internal iliac vessels; 1 cm anterolateral on external iliacs; entire inguinal compartment contoured |
| PTV | 0.5–1 cm expansion from each CTV, depending on setup accuracy, imaging frequency, and IGRT use |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 19.2)
Contouring Atlas: Elective Nodal Regions
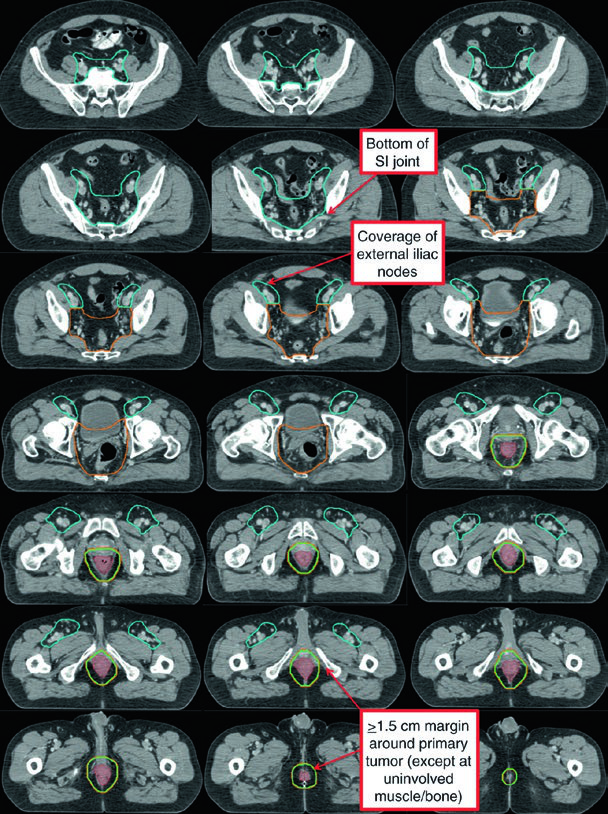
The RTOG anorectal contouring atlas describes three CTV regions that should be included for all patients with anal canal cancer. The Australasian GI Trials Group Atlas details seven elective regions. There is disagreement among the RTOG, AGITG, and BNG guidelines regarding inguinal lymph node contouring — recent data show that 10–29% of involved inguinal nodes fall outside the recommended nodal borders.
| CTV Region (RTOG) | Description |
|---|---|
| CTV-A (perirectal, presacral, internal iliac) | Lower pelvis: inferior border 2 cm below gross disease, including entire mesorectum. Mid pelvis: rectum, mesorectum, internal iliac nodes, 1 cm margin into bladder. Upper pelvis: to the bifurcation of common iliac vessels (~sacral promontory). 7–8 mm margin around internal iliac vessels |
| CTV-B (external iliac) | Border between inguinal and external iliac at the inferior extent of the internal obturator vessels (upper edge of superior pubic rami). 7–8 mm margin, at least 1 cm anteriorly |
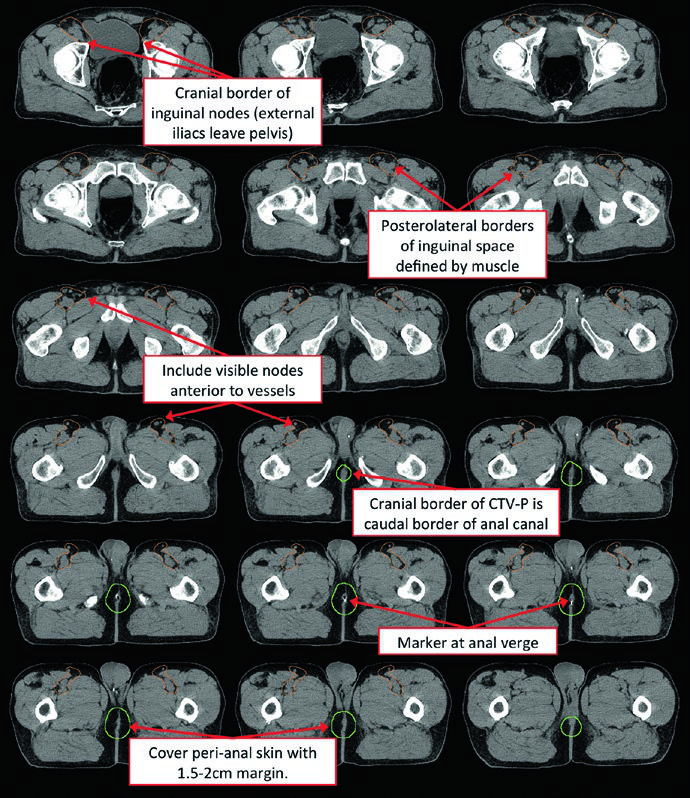
| CTV-C (inguinal) | Inferior extent 2 cm below the saphenous/femoral junction. Entire inguinal compartment contoured including small vessels and lymph nodes |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 19.3 — RTOG Anorectal Contouring Atlas)
To adequately cover the inguinal chain, the recommended approach includes: a 2 cm radial margin around the femoral vessels, 1 cm radial margin around the saphenous/femoral junction, and 3 cm medial/lateral margin along the lower inguinal ligament. The caudal border of the inguinal CTV should be at the level of the anal margin.
Dose and Fractionation: Validated Schemes
There are multiple dose prescription techniques for anal cancer. Current recommendations derive from the treatment plans used in RTOG 9811 and RTOG 0529/Transaustralian protocols.
| Target Volume | RTOG 9811 | RTOG 0529 / Transaustralian |
|---|---|---|
| PTV-P | T1N0: 45–50.4 Gy at 1.8 Gy/fraction T2N0: 50.4 Gy at 1.8 Gy/fraction N+ or T3-T4: 54–59.4 Gy at 1.8 Gy/fraction |
T2N0: 50.4 Gy at 1.8 Gy/fraction N+ or T3-T4: 54 Gy at 1.8 Gy/fraction |
| PTV-N | 54–59.4 Gy at 1.8 Gy/fraction | 50.4 Gy at 1.68 Gy/fraction if node ≤3 cm 54 Gy at 1.8 Gy/fraction if node >3 cm |
| PTV-HR | 45 Gy at 1.8 Gy/fraction | T2N0: 42 Gy at 1.5 Gy/fraction N+ or T3-T4: 45 Gy at 1.5 Gy/fraction |
| PTV-LR | 30.6–36 Gy at 1.8 Gy/fraction (or 40 Gy at 1.6 Gy/fraction with SIB) | Low-risk PTV not used on RTOG 0529 |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 19.5)
Clinical Examples: How Plans Come Together
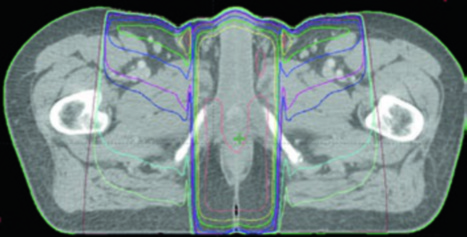
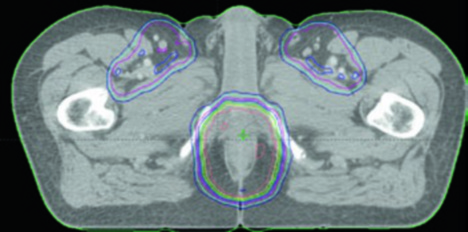
The T2N0 case demonstrates definitive chemoradiotherapy with IMRT: PTV-LR and PTV-HR treated simultaneously to 40 Gy (1.6 Gy/fraction) and 45 Gy (1.8 Gy/fraction) in 25 fractions, respectively. Then PTV-P received a sequential boost to 50.4 Gy (1.8 Gy/fraction) in 28 total fractions.
The T3N1a case with bilateral inguinal involvement had PTV-LR and PTV-HR treated simultaneously to 40 Gy and 45 Gy in 25 fractions. The bilateral inguinal and external iliac nodes were included in CTV-HR due to bilateral inguinal involvement. PTV-P and PTV-N then received a sequential boost to 54 Gy in 30 total fractions.
The third case illustrates a pathologic T1 (1.0 cm) N0M0 squamous cell carcinoma of the perianal skin resected with a close 0.1 cm margin. Adjuvant treatment covered the postoperative bed and inguinal lymph nodes with IMRT: PTV-HR and PTV-P to 45 Gy in 25 fractions, followed by a sequential boost of PTV-HR to 55.8 Gy in 31 total fractions. Even small tumors with close margins demand inguinal coverage.
The planning approach for rectal cancer shares some anatomic principles — particularly regarding mesorectal and internal iliac vessel coverage — but anal cancer specifically demands attention to the inguinal chain.
Plan Assessment and Dose Constraints
Ideally, at least 95% of each PTV should receive 100% of the prescription dose. The maximum dose within the PTV should not exceed 110%. When using sequential boosts, each individual plan should be evaluated separately before the plan sum, checking for hot spots or under-coverage.
| Organ at Risk | Constraints |
|---|---|
| Small bowel | QUANTEC: V15Gy < 120 cc (individual loops); V45Gy < 195 cc (peritoneal cavity) RTOG 0529: V30Gy < 200 cc; V35Gy < 150 cc; V45Gy < 20 cc; Dmax < 50 Gy |
| Large bowel | RTOG 0529: V30Gy < 200 cc; V35Gy < 150 cc; V45Gy < 20 cc |
| Bladder | QUANTEC: Dmax < 65 Gy; V65Gy < 50% RTOG 0529: V35Gy < 50%; V40Gy < 35%; V50Gy < 5% |
| Femoral heads | RTOG 0529: V30Gy < 50%; V40Gy < 35%; V44Gy < 5% |
| Iliac crest | RTOG 0529: V30Gy < 50%; V40Gy < 35%; V50Gy < 5% |
| External genitalia | RTOG 0529: V20Gy < 50%; V30Gy < 35%; V40Gy < 5% |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 19.6 — QUANTEC and RTOG 0529)
Pelvic Bone Marrow: An Emerging Organ at Risk
Pelvic bone marrow is emerging as an important organ at risk for minimizing acute hematologic toxicity in patients receiving concurrent chemoradiotherapy. The pelvic bones serve as a surrogate for the pelvic bone marrow. The structure consists of three sub-sites: lumbosacral spine, ilium, and low pelvis.
Suggested constraints include mean dose < 28 Gy, V10 < 90%, and V20 < 75%. However, these constraints have not been validated prospectively and should not supersede other planning objectives. The lumbosacral spine may be the most active sub-site of the pelvic bone marrow, and limiting dose to this region may be sufficient to reduce hematologic toxicity.
The approach of minimizing pelvic bone marrow dose also applies to other sites treated with pelvic IMRT, such as vulvar cancer and definitive gynecologic malignancies.
Final Considerations for Clinical Practice
Radiation planning for anal cancer requires careful integration of clinical information, multi-modality imaging, and consensus guidelines. The choice between different fractionation schemes — RTOG 9811 versus RTOG 0529 — should consider staging, nodal involvement, and institutional capacity for IMRT with robust IGRT. Compliance with consensus contouring atlases is not optional: adherence to guidelines correlates directly with regional control.
For a comprehensive overview of delineation strategies across all anatomic sites, see our complete guide on target volume delineation and field setup.


