

In This Article
Diagnostic Workup and Primary Site Search
Labeling a cervical node metastasis as an unknown primary demands an exhaustive workup first. In practice, many cases initially classified as CUP reveal their origin when the investigation is aggressive enough.
The minimum evaluation includes a thorough physical examination with cranial nerve testing, fiberoptic visualization of the nasopharynx, oropharynx, larynx, and hypopharynx, plus high-resolution contrast-enhanced CT. A detailed skin and scalp examination is essential — cutaneous malignancies are real differential diagnoses.
Patient history deserves careful attention. Risk factors for thoracic, gynecologic, or gastrointestinal cancers should be evaluated, as cervical adenopathy may represent infraclavicular disease. PET/CT adds sensitivity for detecting occult primaries but must be performed before biopsy to reduce false-positive inflammatory uptake. Panendoscopy remains a useful complement.
For a comprehensive overview of all head and neck sites, see our complete guide on target volume delineation in radiation therapy.
HPV, EBV Testing and Directed Biopsy
HPV and EBV testing directly guides pharyngeal coverage strategy and has changed how these tumors are classified. In the AJCC 8th edition, HPV-positive nodes are staged as T0 oropharynx, while EBV-positive nodes are classified as T0 nasopharynx. This distinction carries immediate planning implications.
Directed biopsies of all suspicious lesions along the pharyngeal axis are mandatory. Blind biopsies of normal-appearing mucosa have been traditionally recommended but only occasionally identify the primary. A more effective approach: transoral tongue base mucosectomy (lingual tonsillectomy) combined with at least ipsilateral palatine tonsillectomy detects roughly 80% of unknown primary cases, particularly HPV-related ones. Some centers perform bilateral palatine tonsillectomies and may omit lingual tonsillectomy.
This matters because HPV-positive patients may need only oropharyngeal irradiation. EBV-positive patients — especially those of Asian ethnicity — may require treatment to the nasopharynx alone. The pattern of lymph node spread further refines the decision about pharyngeal coverage extent.
Treatment Decision: Single vs. Combined Modality
Patients with a single ipsilateral lymph node measuring 3 cm or smaller without extranodal extension may be candidates for single-modality therapy — surgery or radiation alone. This is a relatively favorable scenario that allows sparing patients the morbidity of combined treatment.
When extended-field IMRT is planned, CT simulation with IV contrast is essential for delineating involved lymph nodes. The thermoplastic mask should immobilize the head, neck, and shoulders — not just the head and neck — to ensure positional reproducibility across fields extending inferiorly.
In the postoperative setting, concurrent chemotherapy should be considered when extracapsular extension (ECE) is present. In the definitive setting, advanced nodal disease is an indication for concurrent chemotherapy. The dissected neck should receive 60–66 Gy in 2 Gy fractions. Related articles on other head and neck subsites provide complementary detail on site-specific anatomy and contouring.
Target Volumes and Pharyngeal Mucosal Coverage
Bilateral neck treatment with coverage of pharyngeal mucosal areas at risk is the standard recommendation. Some institutions have treated the ipsilateral neck alone; however, neck relapse and distant metastasis rates appear higher than with comprehensive radiotherapy.
Traditionally, the entire pharynx was included. IMRT allows more specific targeting of pharyngeal portions most likely to harbor the primary, sparing normal structures and minimizing side effects. The pharyngeal extent to irradiate must be determined case by case. When in doubt, the entire pharynx should be treated. For cases with full TORS evaluation, emerging data suggests the pharyngeal axis may be safely spared, though this needs prospective validation.
Suggested Target Volume Definitions
The table below summarizes recommended volume definitions for unknown primary head and neck cancer.
| Volume | Definition and Description |
|---|---|
| GTV70 | All lymph nodes ≥ 1 cm in short axis, significantly FDG avid, or biopsy-positive. Contour any equivocal nodes as GTV. GTV = CTV70 |
| PTV70 | GTV70 + 3–5 mm depending on institutional daily positioning accuracy |
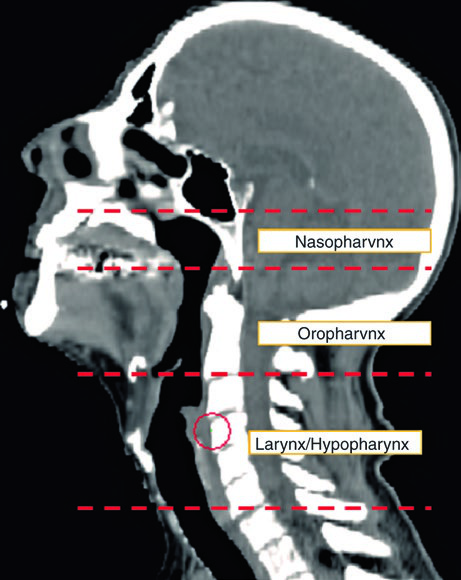
| CTV nasopharynx | From skull base (superiorly) to soft palate (inferiorly). Anteriorly from the posterior choana to the posterior pharyngeal wall. Laterally: adequate coverage of the fossa of Rosenmüller |
| CTV oropharynx | From soft palate surface (superiorly) to floor of vallecula or hyoid bone (inferiorly). Tongue base covered anteriorly — oral tongue margin not necessary. Tonsils adequately covered laterally. Entire posterior pharyngeal wall included |
| CTV larynx & hypopharynx | From hyoid bone (superiorly) to bottom of cricoid cartilage (inferiorly) |
| PTV mucosa | 3–5 mm expansion on mucosal surface CTVs depending on institutional positioning accuracy |
Note: Suggested dose to gross disease: 70 Gy in 33–35 fractions. Dose to mucosal surfaces at risk: 54–60 Gy. Postoperative dissected neck: 60–66 Gy in 2 Gy fractions. Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 10.1)
For the node-positive neck, cervical levels Ib–V and retropharyngeal lymph nodes should be included. The contralateral neck receives prophylactic dose to levels II–IV and retropharyngeal nodes. Some authors advocate sparing the larynx when no low lymph nodes are involved.
Postoperative Case: Practical Contouring
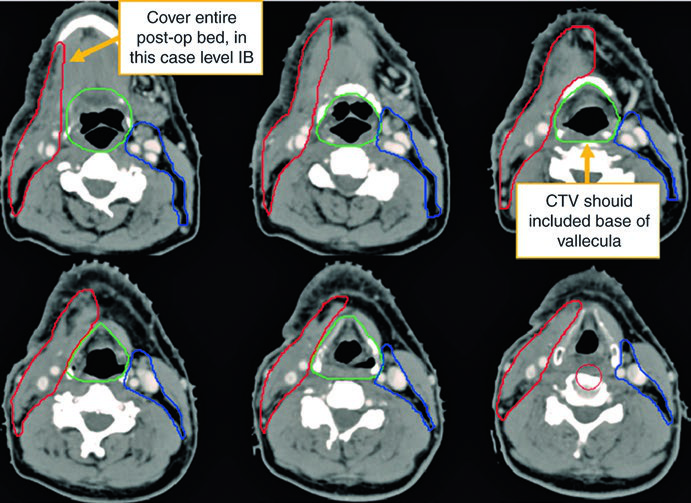
The first case illustrates a 62-year-old male with TxN2a unknown primary who underwent bilateral tonsillectomy and right neck dissection revealing a single 4.6 cm level II lymph node.
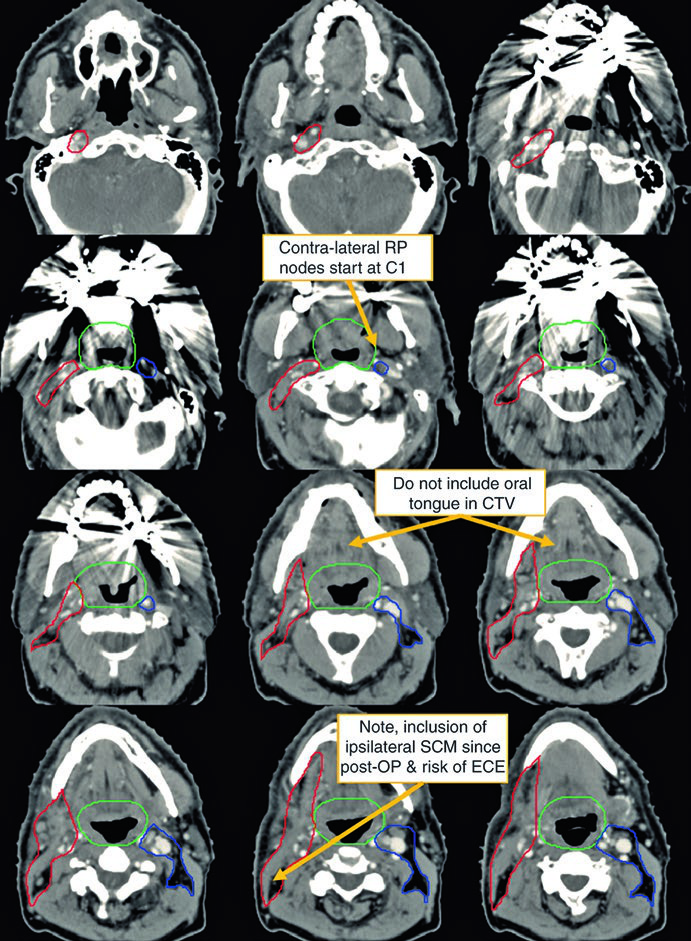
Notice the difference between the contouring on the operated (ipsilateral) neck versus the contralateral side. The CTV66Gy (red) covers the high-risk surgical bed; the CTV54-60Gy (green) covers pharyngeal mucosa at risk for harboring the primary; and the CTV54Gy (blue) provides prophylactic coverage of the contralateral neck. This asymmetry reflects the principle of dose escalation according to actual risk.
Sagittal views (Fig. 10.2) are particularly helpful for confirming correct craniocaudal extent of mucosal volumes — nasopharynx, oropharynx, and larynx/hypopharynx — and ensuring no gaps between adjacent CTVs. The radiographic isocenter serves as the geometric reference for planning.
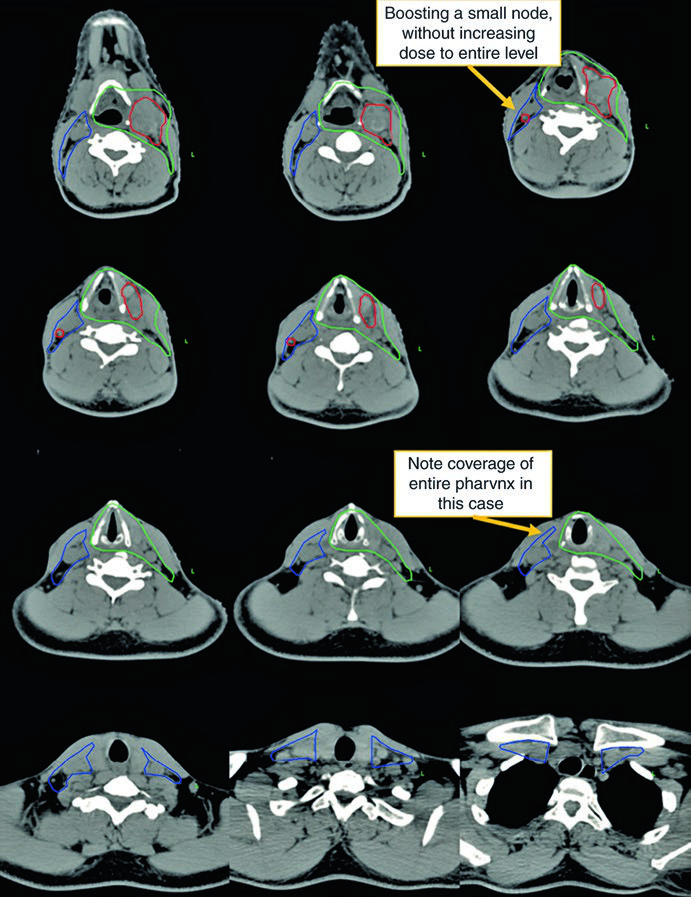
Definitive Case: Bilateral HPV-Negative Disease
The second case demonstrates a more aggressive scenario: a 50-year-old male with TxN2c, open biopsy of a left-sided node showing extranodal extension, HPV ISH and p16 negative. He received definitive chemoradiotherapy.
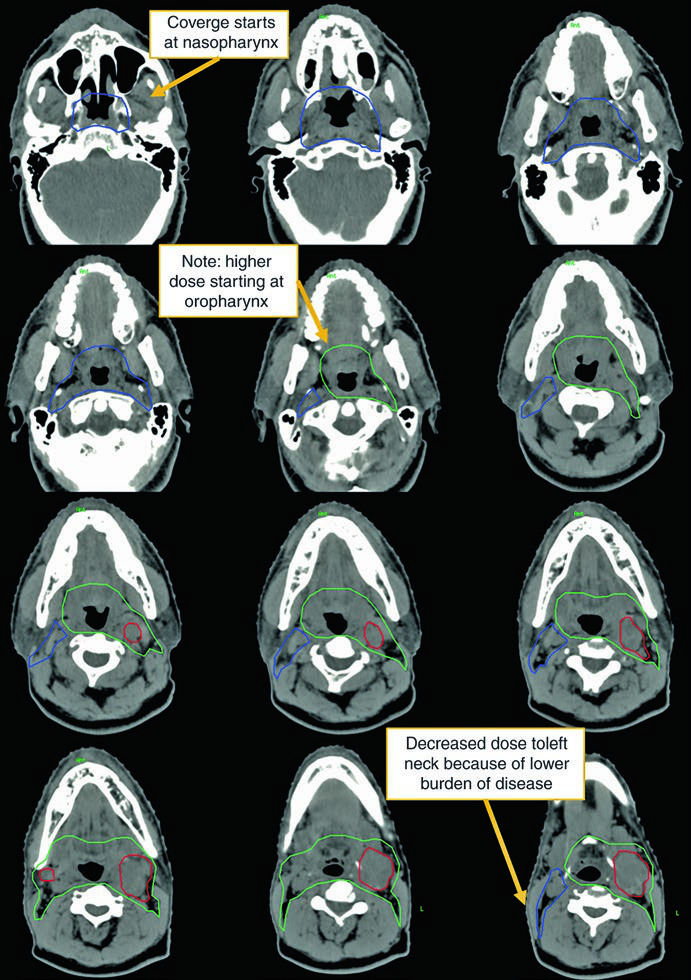
Here the CTV70Gy (red) encompasses bilateral gross disease; the CTV60Gy (green) covers pharyngeal mucosa at risk; and the CTV54Gy (blue) includes the entire bilateral neck prophylactically. HPV negativity justifies comprehensive pharyngeal coverage — without viral guidance toward a specific subsite, risk is distributed along the entire mucosal axis.
ECE in this case reinforces the indication for concurrent chemotherapy. The dose of 70 Gy to gross disease and 54–60 Gy to at-risk mucosa follows the standard dose-escalation paradigm.
Managing unknown primary head and neck cancer requires aggressive investigation before diagnosis, personalized treatment decisions based on HPV/EBV status and nodal disease extent, and careful RT planning that balances adequate coverage with normal tissue preservation. For the full picture of all head and neck sites covered in this series, visit the complete guide on target volume delineation.


