

Planning Principles for Soft Tissue Sarcoma Radiotherapy
Soft tissue sarcoma (STS) demands a fundamentally different approach to target volume delineation compared with most solid tumors. The anatomic location, tumor size, depth relative to the superficial fascia, and histopathological features dictate the entire management strategy. STS characteristically invades along the longitudinal axis within muscle and remains confined to the compartment of origin — a biological behavior that directly shapes how we design treatment volumes.
Suspicious peritumoral edema — best visualized on T2-weighted MRI — may harbor microscopic disease and extends predominantly in the craniocaudal dimension. In routine practice, this edema should be encompassed within the radiotherapy target volume. Natural barriers to tumor spread, including bone, interosseous membrane, and major fascial planes, must be exploited in tissue-preserving radiotherapy planning, particularly for extremity lesions.
For a comprehensive overview of all anatomical sites and delineation principles, see our complete guide to target volume delineation in radiotherapy.
Preoperative Target Volume Definition in Extremity STS
For preoperative planning, CT simulation imaging fused with MRI should be performed with the patient in the treatment position whenever feasible. T1-weighted contrast-enhanced MRI is the preferred sequence for delineating the gross tumor volume (GTV), while T2-weighted images demonstrate the full extent of peritumoral edema that often extends several centimeters along the longitudinal axis.
The standard preoperative dose is 50 Gy in 25 fractions at 2 Gy per fraction. The CTV50 includes the GTV with a 4-cm margin longitudinally and 1.5 cm radially, limited to but including any anatomic barrier to tumor spread such as bone or fascia. Suspicious peritumoral edema should be contoured separately and included with an adequate margin of usually 1 to 2 cm. The PTV adds 0.5 to 1.0 cm to the CTV, determined by institutional protocols.
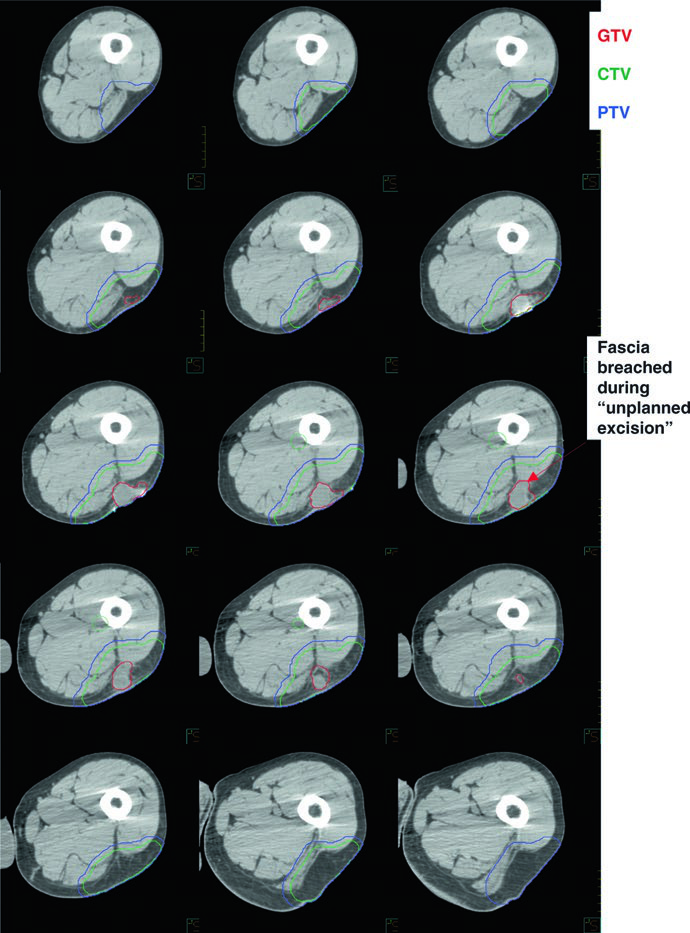
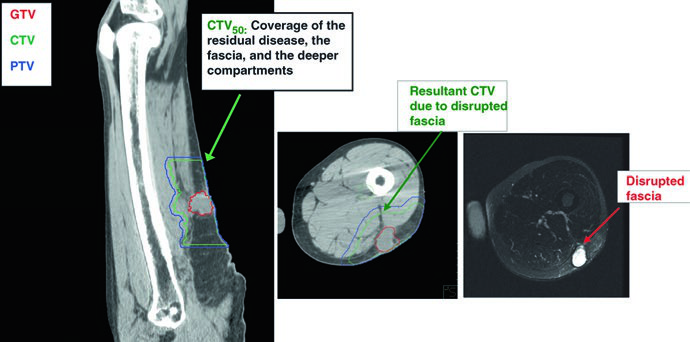
In cases of “unplanned excision” — a surgical error where margins turn out positive — the target volume must generously include the postoperative GTV or any residual gross disease, all surgically manipulated and disturbed tissues, violated fascia, plus 4 cm longitudinally and 1.5 cm radially up to the nearest anatomic barrier.
Suggested Target Volumes for Preoperative Extremity STS
The following table outlines contouring recommendations for the preoperative setting, emphasizing direction-specific margins and the critical role of peritumoral edema.
| Volume | Definition and Description |
|---|---|
| GTV | All gross disease on physical examination and imaging. T1-weighted contrast-enhanced MRI preferred. Co-registration of MRI and planning CT facilitated by immobilizing the patient in the treatment position. |
| CTV50 | GTV + 4-cm margin longitudinally and 1.5 cm radially, limited to but including anatomic barriers (bone, fascia). Suspicious peritumoral edema (T2-MRI) contoured separately with 1–2 cm margin. For unplanned excisions: GTVpostop + all disturbed tissues + violated fascia + 4 cm longitudinal / 1.5 cm radial margins. |
| PTV50 | CTV50 + 0.5–1.0 cm per institutional protocol. |
Suggested dose: 2.0 Gy/fraction to 50 Gy. Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 32.1).
Postoperative Planning: Reconstructing the GTV and Managing Boost Volumes
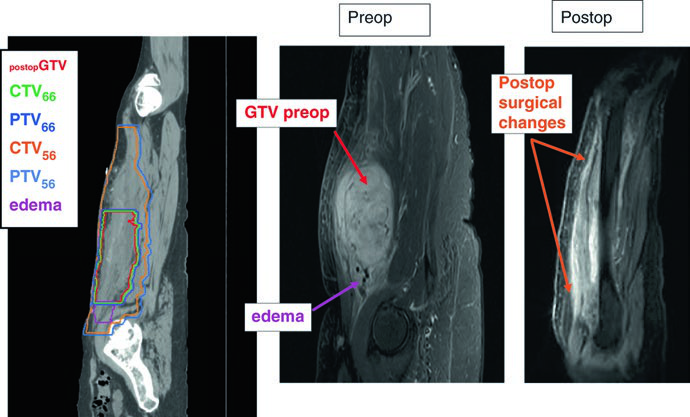
After complete surgical resection, there is no GTV to delineate. The planning strategy shifts entirely: the location of the original tumor (GTVpostop) must be recreated on the planning CT dataset using preoperative CT/MRI imaging. This step is non-negotiable — without it, adequate coverage of the original tumor bed is impossible.
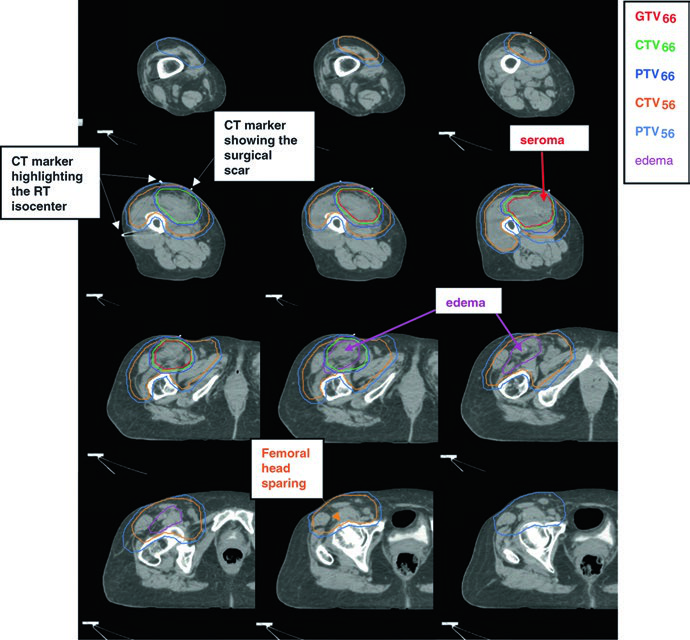
The standard postoperative dose is 66 Gy (60 Gy may be acceptable for clear margins in low-grade tumors). The recommended technique is a simultaneous integrated boost (SIB): the CTV66 receives the high dose to the highest-risk region, while the CTV56 covers the peripheral subclinical area at 1.69 Gy per fraction to 56 Gy. For unresectable residual gross disease, 70 Gy in 2 Gy fractions is ordinarily used, depending on regional tolerance.
Communication with the surgeon and review of surgical and pathology reports are essential to decide whether seroma, lymphocele, or hematoma should be included in the volume. The surgical scar and drain sites are typically included within the CTV56. When the subcutaneous tissues have been contaminated, bolus may be applied over the scar for a component of the treatment (e.g., the first 50 Gy).
Suggested Target Volumes for Postoperative Extremity STS
| Volume | Definition and Description |
|---|---|
| GTVpostop | Identifies the original tumor site. Import presurgical imaging when contouring on the RT planning CT to ensure adequate coverage of original tumor extent. |
| CTV66 | GTVpostop + immediate surgical change area with 1–2 cm longitudinal and 1.5 cm transverse margin. May include surgically disturbed tissues, scars, and drain sites. |
| PTV66 | CTV66 + 0.5–1.0 cm. |
| CTV56 | GTVpostop + 4 cm longitudinally and 1.5 cm radially to anatomic barriers. Surgically disrupted tissue, scars, and drain sites with 1–2 cm margin if not in CTV66. Peritumoral edema contoured separately; recent postoperative MRI recommended. |
| PTV56 | CTV56 + 0.5–1.0 cm. |
SIB technique: CTV66 at 2.0 Gy/fx to 66 Gy; CTV56 at 1.69 Gy/fx to 56 Gy. Alternative: sequential shrinking-field technique with 50 Gy + 16 Gy boost. Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 32.2).
Extensive Edema and Dual-Isocenter IMRT Technique
Peritumoral edema in extremity sarcomas can be remarkably extensive. A striking example from the textbook describes a grade 2 myxofibrosarcoma of the lateral thigh with massive longitudinal edema, producing a PTV measuring 42 cm — well beyond the maximum field size for single-isocenter techniques on most linear accelerators.
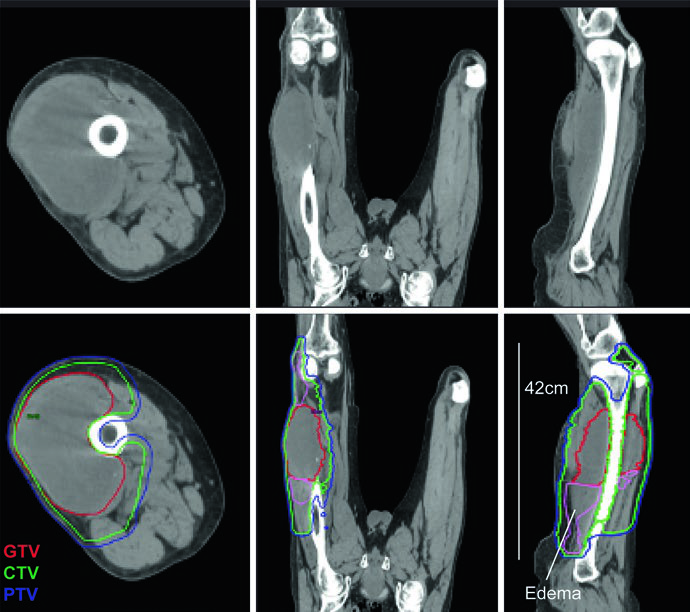
The solution involved a dual-isocenter IMRT technique, with isocenters strategically placed near the center of each adjoining subvolume and co-optimized to ensure uniform PTV coverage at the junction. This scenario underscores why complete edema mapping on T2-MRI is essential before simulation: underestimating the edema extent risks inadequate coverage. Sagittal MRI is particularly valuable for delineating craniocaudal spread.

One critical detail: the CTV is limited by bone throughout the target. STS respects barriers such as cortical bone and interosseous membranes, so there is no need to expand the volume into bone. This tissue-sparing principle meaningfully reduces late toxicity. Additional considerations for younger patients are discussed in our article on pediatric sarcoma delineation.
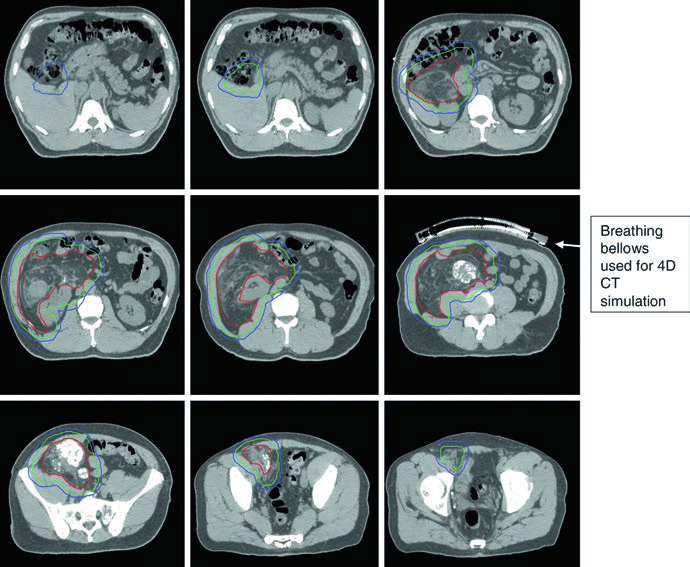
Retroperitoneal Sarcoma: A Distinct Challenge
Retroperitoneal sarcomas pose entirely different challenges than extremity tumors. These lesions frequently grow to enormous volumes, initially displacing and eventually invading adjacent organs. The recommended dose is 50 Gy in 25 fractions to 50.4 Gy in 28 fractions, delivered exclusively in the preoperative setting.
Radial margins in the retroperitoneum are more conservative (0.5–2.0 cm) while maintaining 2 cm longitudinally, because critical adjacent anatomy imposes hard limits. When the tumor approximates an intact liver, only 0.5 cm of liver parenchyma is included in the CTV. Posteriorly, 2-cm margins are typically used to cover fatty tissues and vessels. The ipsilateral kidney may be sacrificed provided the contralateral kidney demonstrates acceptable function — in that case, dose to the uninvolved kidney should be kept as low as reasonably achievable.
Suggested Target Volumes for Retroperitoneal STS
| Volume | Definition and Description |
|---|---|
| GTV | All gross disease on physical examination and imaging. |
| CTV | GTV + 2-cm margin longitudinally and 0.5–2.0 cm radially, limited by anatomic barriers and critical anatomy. If tumor approximates intact liver, 0.5 cm of liver included. 2-cm posterior margins for fatty tissues and vessels. Ipsilateral kidney may be sacrificed if contralateral function is adequate. |
| PTV | CTV + 0.5 cm per institutional protocol. |
OAR: small bowel, liver, spinal cord, and lungs. 4DCT simulation encouraged. Dose: 50 Gy/25 fx to 50.4 Gy/28 fx. Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 32.3).
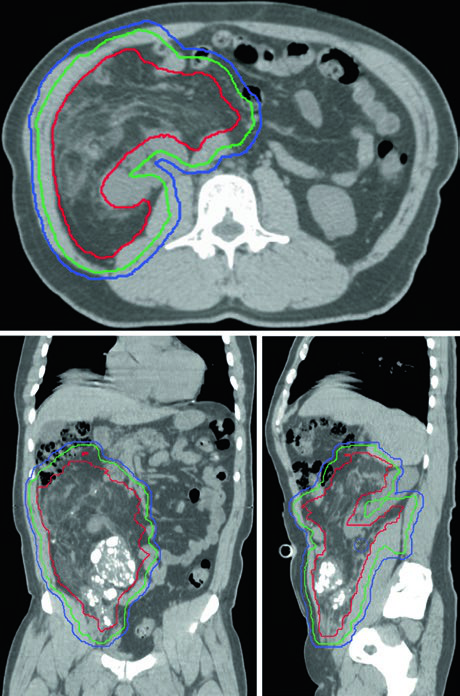
4DCT simulation is strongly recommended in the retroperitoneum, where respiratory motion can shift the tumor and adjacent organs. Multifocal intratumoral calcifications, when present, serve as excellent fiducial surrogates for daily image guidance during targeted IMRT. The bowel displacement by the tumor itself is, somewhat paradoxically, an advantage of the preoperative approach: with the tumor still in situ, bowel loops are naturally pushed away from the treatment field.
Practical Pearls and Common Pitfalls
The TNM staging classification changed in its eighth edition, introducing different size thresholds for different anatomic sites and eliminating depth from the classification criteria. While this doesn’t substantially alter delineation principles, it remains important when staging patients.
CT simulation with 2.0-mm slice thickness is the standard for all cases described in the text. MRI co-registration should be performed whenever possible — in both preoperative and postoperative scenarios. For postoperative cases, both preoperative and postoperative MRI should be imported and co-registered with the planning CT to appreciate both the original tumor extent and the surgical changes.
Several details deserve particular attention: a 5-mm bolus plug may be needed to fill soft-tissue defects (as in the case of a skin graft over periosteum with a positive deep margin); the femoral head should be respected as a dose-limiting OAR wherever the CTV approaches it; and in unplanned excision cases, radial margins approximate postoperative margins to account for the absent GTV and contamination from intralesional surgery. For insights into how similar barrier-respecting principles apply to other disease sites, such as lymphoma field design, explore the other dedicated articles in our series.


