

Who is Kirsten Donald
Kirsten Donald, a pediatrician trained in child neurology at the University of Cape Town, is now one of the leading global voices on using MRI to understand how environmental factors shape brain development. At ISMRM 2026, she returned to the spotlight to discuss how the longitudinal Drakenstein Child Health Study has been mapping the relationship between early adversity and brain structure in South African children — work that is rewriting textbooks on neural plasticity in the first one thousand days of life.
Donald heads the Division of Paediatric Neurology at Red Cross War Memorial Children’s Hospital, is an associate professor of pediatrics at UCT, and is the principal investigator for the neuroimaging arm of Drakenstein. Her career mission is clear: use medical imaging to see — and ideally intervene on — the factors that compromise brain development before they crystallize into adult psychiatric or neurological diagnoses.
The Drakenstein study and MRI’s role
The Drakenstein Child Health Study is a prospective cohort of roughly 1,000 mother–child pairs recruited from low-income communities near Cape Town, South Africa. Children are followed from before birth, with repeated assessments that include brain MRI at critical points — neonatal, two years, five years, and early adolescence. The dataset is unique: it covers a population exposed to factors rarely captured in Northern Hemisphere cohorts, including high-prevalence prenatal alcohol exposure, treated maternal HIV, tuberculosis, malnutrition, and domestic violence.
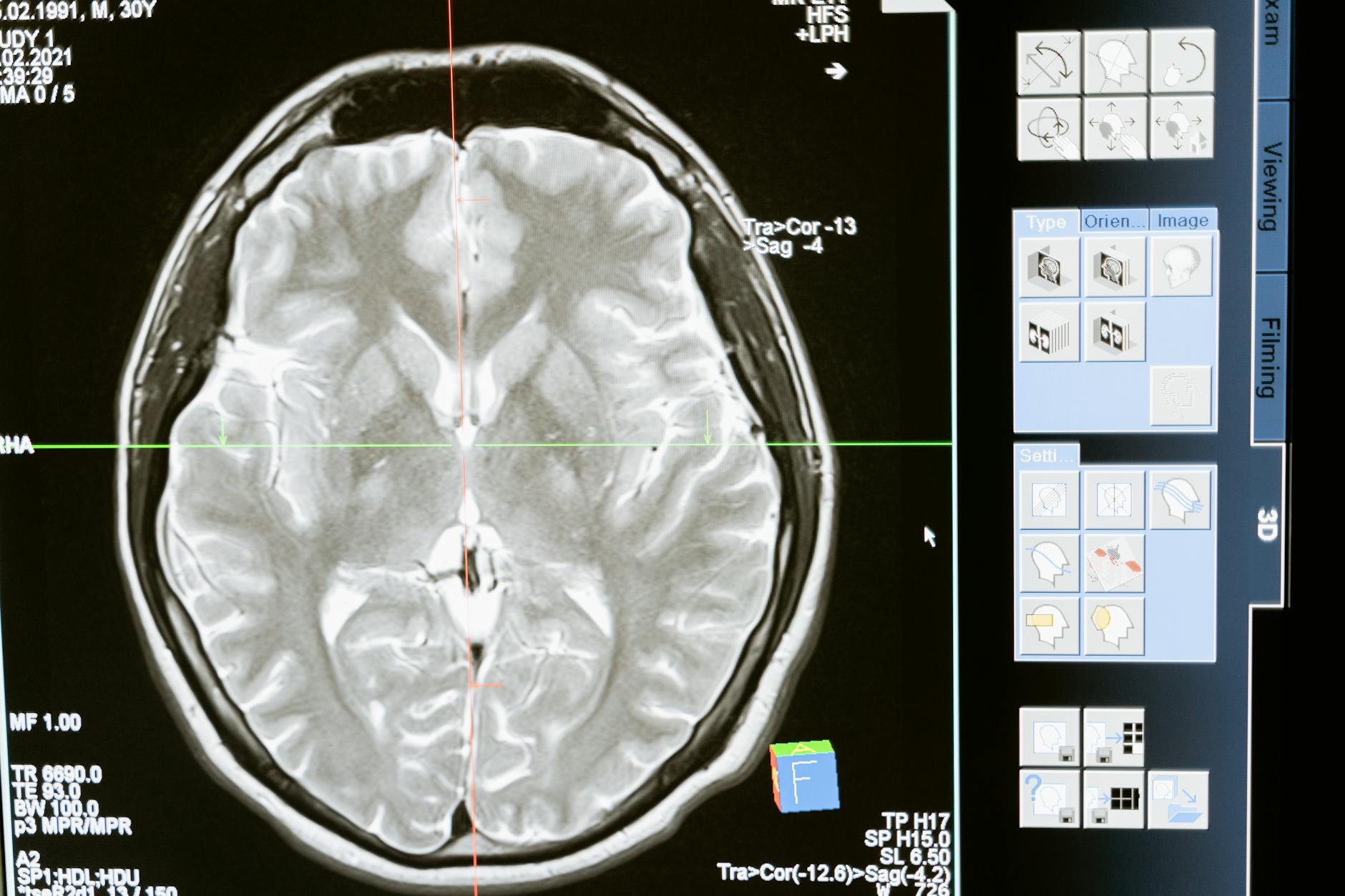
MRI is the technical backbone of that work. Using structural (T1, T2) sequences, diffusion (DTI), and at times resting-state functional MRI, the team maps gray-matter volumes, white-matter tract integrity, and connectivity — biomarkers that correlate with cognitive and behavioral scores at follow-up.
Findings that are changing practice
Three result sets stand out:
- Prenatal alcohol exposure: even at “moderate” levels, the group sees volumetric reduction in the cerebellum, corpus callosum, and hippocampus. The finding strengthens the public-health message against alcohol use during pregnancy — there is no established safe threshold.
- Maternal HIV exposure: children born to treated, HIV-positive mothers, while uninfected, show distinct myelination patterns in early weeks, suggesting intrauterine environmental effects beyond classical virology.
- Socioeconomic adversity: poverty, food insecurity, and domestic violence correlate with changes in functional connectivity and prefrontal area development — a biological substrate for behavioral impacts documented for decades.
Implications for radiologic practice
Donald and the South African group’s work reinforces a point that pediatric radiologists increasingly know: MRI in children is not only disease diagnosis — it is also a tool for monitoring and risk stratification. For the clinical radiologist, that means paying closer attention to subtle findings on neonatal and pediatric MRI, and talking more often with pediatricians and pediatric neurologists about “subclinical” findings with prognostic relevance.
The parallel with discussions on pediatric MRI safety is direct: as younger children enter MRI earlier and more frequently, Zone-IV protocol rigor becomes as important as acquisition quality.
MRI in low-resource settings: lessons from Drakenstein
One of the most admired aspects of the project is showing that high-quality neuroimaging research is possible outside traditional hubs (Boston, London, Tokyo). The group invested in local technical training, partnerships with European and North American universities, and a modest yet adequate infrastructure (3T MRI shared with hospital clinical practice). For services across the Global South, the model is inspiring: cutting-edge pediatric research does not require exclusive Big Science.
ISMRM 2026 itself brought advances that connect to this agenda. Sessions on amplified MRI for brain pulsatility and radiomics in breast oncology showed that the future of MRI runs through integrating advanced functional techniques, AI, and carefully characterized longitudinal cohorts — exactly the Drakenstein formula.
What to expect next
Donald signals that the next frontier is clinical translation: turning imaging biomarkers identified in epidemiological studies into screening tools that guide early intervention — occupational therapy, family support, parental education. The challenge is methodological (defining clinical cutoffs for subtle neuroimaging changes) and ethical (avoiding premature labeling of children based on MRI).
For radiologists worldwide, the lesson is twofold: a growing MRI footprint in following at-risk children, and the opportunity to plug into global research networks that focus on populations historically underrepresented in imaging cohorts. Brazil, with its diverse pediatric base and growing 3T fleet, is well placed to join that wave.
The Drakenstein model also has a quieter contribution that often gets missed: it has trained a generation of African radiographers, MR physicists, and pediatric radiologists who now staff the very services that publish from the region. That capacity-building loop is the long-term return on investment that pure-imaging metrics rarely capture, and it is precisely the kind of soft infrastructure that determines whether advanced MRI techniques diffuse beyond a handful of academic hubs.
Looking ahead, several open questions will shape the next decade of work like Donald’s: how to standardize pediatric MRI acquisition across very different scanners, how to share neuroimaging data ethically and securely across jurisdictions, and how to design clinical trials that test whether MRI-guided early interventions actually move outcomes. ISMRM has been an unusually open forum for those discussions, and Donald’s session was a reminder of why annual meetings still matter when so much of science has moved online.
Source: AuntMinnie — ISMRM: Kirsten Donald on using MRI to improve children’s lives


