

Target Volume Delineation in Gastric Cancer
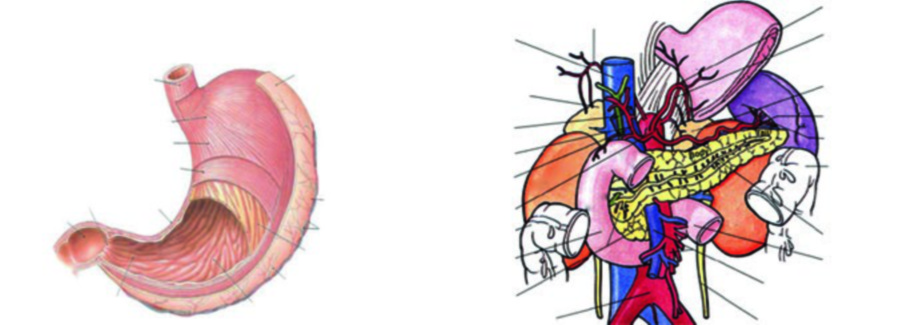
Gastric cancer radiotherapy planning demands meticulous attention to the post-surgical anatomy and nodal drainage patterns. The stomach extends from the gastro-esophageal junction (GEJ) to the pylorus, with the greater curvature forming the left convex border and the lesser curvature forming the right concave border. It is divided into four anatomical regions — cardia, fundus, body, and antrum — and its wall has five histological layers: mucosa, submucosa, muscularis externa, subserosa, and serosa. For a comprehensive overview of all anatomical sites covered in this series, see our complete guide on target volume delineation.
Regarding primary location, tumors arising from the GEJ, cardia, and fundus account for approximately 35% of cases; body tumors represent about 25%; and antral and distal stomach tumors make up roughly 40%. This distribution directly impacts planning, since CTV volumes change substantially depending on the subsite of origin.
In terms of local extension, the tumor can directly invade the liver, duodenum, pancreas, transverse colon, omentum, and diaphragm. Proximal tumors frequently spread upward into the esophagus. Perineural invasion is another route of dissemination that cannot be overlooked.
Lymph Node Stations and Patterns of Spread
Lymph node involvement in gastric cancer is remarkably prevalent — up to 80% of patients already have nodal metastases at diagnosis. In practice, this means that delineation of nodal volumes is just as critical as coverage of the tumor bed itself.
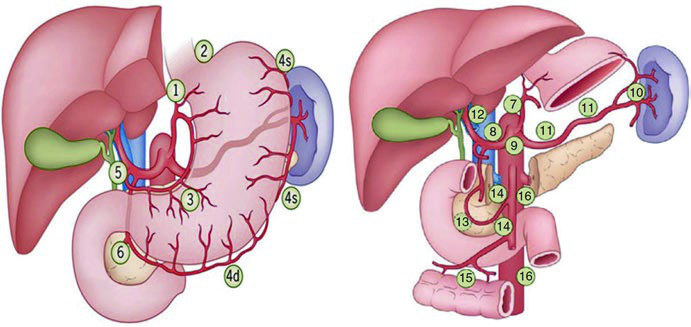
The Japanese classification (JRSGC) organizes the stations into four tiers. The following table faithfully reproduces the distribution published in the textbook, with the anatomical correspondence of each station.
Lymph Node Stations — JRSGC Classification
| Group | Station | Description |
|---|---|---|
| N1 | 1 | Right cardial nodes |
| N1 | 2 | Left cardial nodes |
| N1 | 3 | Nodes along the lesser curvature |
| N1 | 4 | Nodes along the greater curvature |
| N1 | 5 | Suprapyloric nodes |
| N1 | 6 | Infrapyloric nodes |
| N2 | 7 | Nodes along the left gastric artery |
| N2 | 8 | Nodes along the common hepatic artery |
| N2 | 9 | Nodes along the celiac axis |
| N2 | 10 | Nodes at the splenic hilum |
| N2 | 11 | Nodes along the splenic artery |
| N3 | 12 | Nodes in the hepatoduodenal ligament |
| N3 | 13 | Nodes at the posterior aspect of the pancreatic head |
| N3 | 14 | Nodes at the root of the mesenterium |
| N4 | 15 | Nodes in the mesocolon of the transverse colon |
| N4 | 16 | Para-aortic lymph nodes |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 15.1). Adapted from Hartgrink & Van De Velde (2005).
Clinically, proximal tumors and those at the GEJ tend to spread to the lower paraesophageal nodes. Body tumors can involve virtually every station. Distal stomach and antral tumors have a greater tendency to involve periduodenal and porta hepatis nodes. This dissemination logic forms the basis for nodal CTV selection.
Diagnostic Workup for Target Delineation
Before RT planning, it is imperative to review the surgical and pathology reports and discuss with the surgeon to identify areas at highest risk for recurrence. The type of operation — total versus partial gastrectomy — must be noted, as it fundamentally changes the post-operative anatomy.

Preoperative CT scans should be reviewed to identify the location of the primary tumor and involved regional lymphatics. It is worth noting that FDG PET alone is not adequate for staging gastric cancer, since diffuse and mucinous subtypes exhibit low FDG uptake — a common diagnostic pitfall.
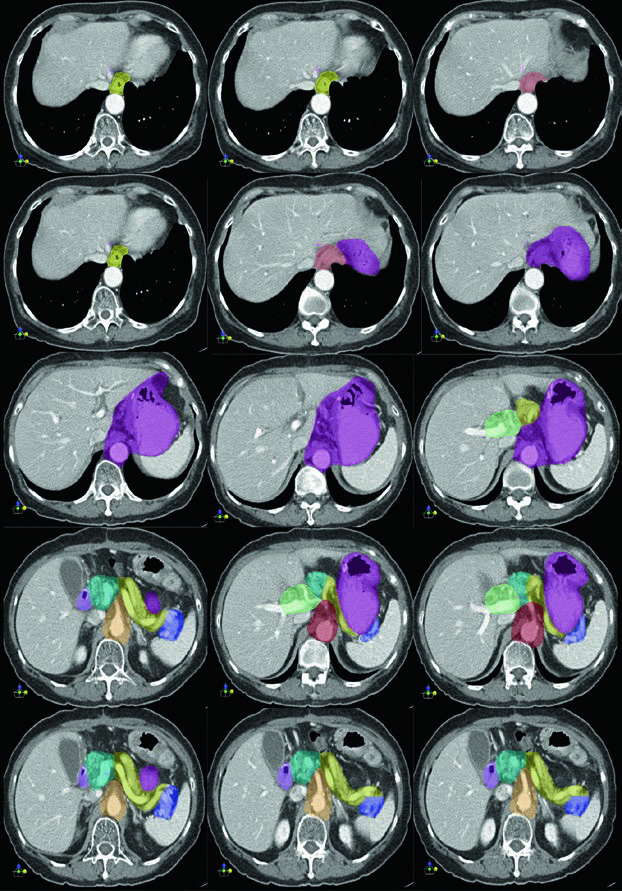
A pre-radiation quantitative renal perfusion study to evaluate relative bilateral kidney function should be considered. The post-operative diagnostic CT scan with oral and intravenous contrast is required, with precise identification of: the esophagus and gastric remnant, the anastomosis (gastrojejunal or esophagojejunal), the duodenal stump, the porta hepatis, the splenic hilum, the pancreas, and the celiac artery and superior mesenteric artery.
General Planning Principles and Adjuvant CTV
Patients should fast for 2–3 hours before the simulation CT and before each treatment fraction. The planning CT, with 3–5 mm slice thickness, should be acquired with the patient supine with arms overhead, extending from the top of the diaphragm (or the carina for GEJ/cardia tumors) to the bottom of L4.
Immobilization with a vacuum bag such as VacLok is recommended for IMRT. Intravenous contrast is preferred to demonstrate blood vessels and guide CTV delineation, particularly for lymph node volumes.
Target Volume Definitions
| Volume | Definition and Description |
|---|---|
| GTV | Gross residual disease defined by CT imaging and surgical findings |
| PTV (residual disease) | Residual GTV / positive margins + 1.5 cm. Cone-down boost after 45 Gy to a total dose of 50.4–54 Gy in 1.8 Gy/fraction |
| CTV45 | Coverage of nodal groups according to subsite (Tables 15.5–15.8). Also includes remnant stomach, anastomosis (gastrojejunal, esophagojejunal), duodenal stump |
| PTV45 | CTV45 + 1 cm margin. A larger margin may be required for organ motion and setup uncertainties |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 15.2)
Three areas must be identified as CTV for adjuvant radiotherapy: the gastric tumor bed, the anastomosis or stumps, and the regional lymphatics. Additionally, the hepatogastric ligament should preferably be treated in all cases, as it carries a high risk of recurrence — it represents the portion of the lesser omentum running between the lesser curvature and the liver, containing the left and right gastric nodes that are not always completely removed at surgery.
The recommended total dose for adjuvant RT with concurrent chemotherapy is 45 Gy in 25 fractions using high-energy (≥6 MV) photons. Boosts to 50.4–54 Gy for positive margins or residual disease should be given, provided doses to surrounding critical organs remain within tolerance.
Impact of T and N Category on Treatment Volumes
| TN Category (AJCC 8th Edition) | Remaining Stomach | Tumor Bed | Nodes |
|---|---|---|---|
| T1-2N0 (not into subserosa) | No | No | No |
| T2N0 (into subserosa) | Variable | Yes | No |
| T3N0 | Variable | Yes | No |
| T4N0 | Variable | Yes | Variable |
| T1-2N+ | Yes | No | Yes |
| T3-4N+ | Yes | Yes | Yes |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 15.4). Adapted from Clinical Radiation Oncology, 4th Edition.
CTV by Subsite: Gastro-Esophageal Junction
For GEJ tumors, the remaining stomach should be included provided it allows exclusion of two-thirds of the right kidney. Tumor bed coverage depends on T stage: for T2N0 with subserosal invasion, the medial left hemidiaphragm and adjacent body of the pancreas are included. For T3N0, the approach is similar. For T4N0, sites of adherence with a 3–5 cm margin are added.
Nodal volumes for GEJ tumors include perigastric (PG), perioesophageal (PEN), celiac (CN), and mediastinal (MN) nodes, depending on N status. A 4 cm margin of the esophagus should be included in the CTV for GEJ tumors. Optional nodal inclusion for T2-3N0 is acceptable when adequate D2 dissection with at least 10–15 nodes examined has been performed.
CTV by Subsite: Cardia and Proximal Third
For cardia and proximal third tumors, the remaining stomach should be included while sparing two-thirds of one kidney, usually the right. The tumor bed for T2N0 includes the medial left hemidiaphragm and adjacent body of the pancreas, with or without the tail. In T1-2N+ disease, nodal volumes expand to include PG, CN, splenic, suprapancreatic (SP), with possible mediastinal (MN), pancreaticoduodenal (PD), and porta hepatis (PH) nodes. Notably, PD and PH nodes carry low risk when nodal positivity is minimal (1–2 positive nodes with 10–15 examined).
CTV by Subsite: Body and Middle Third
In body tumors, the remaining stomach is always included, sparing two-thirds of one kidney. The tumor bed for T2-3N0 corresponds to the body of the pancreas with or without the tail. Nodal volumes for T1-2N+ disease include PG, CN, splenic, SP, PD, and PH — essentially all relevant perigastric and retroperitoneal stations.
CTV by Subsite: Antrum, Pylorus, and Distal Third
For antral and pyloric tumors, the remaining stomach is included while sparing two-thirds of the left kidney (note: the opposite side compared to GEJ). The tumor bed for T2-3N0 encompasses the head of the pancreas with or without the body, plus the first and second portions of the duodenum. Nodal volumes for T1-2N+ include PG, CN, SP, PD, and PH, with optional splenic hilum coverage.
Clinical Cases: CTV in Practice
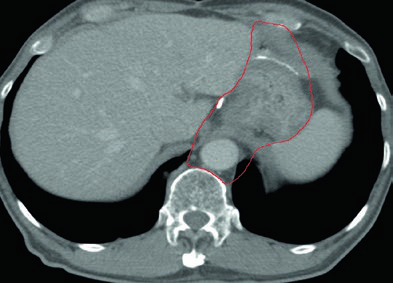
Case 1: T1N1M0 Cardia Adenocarcinoma — Total Gastrectomy
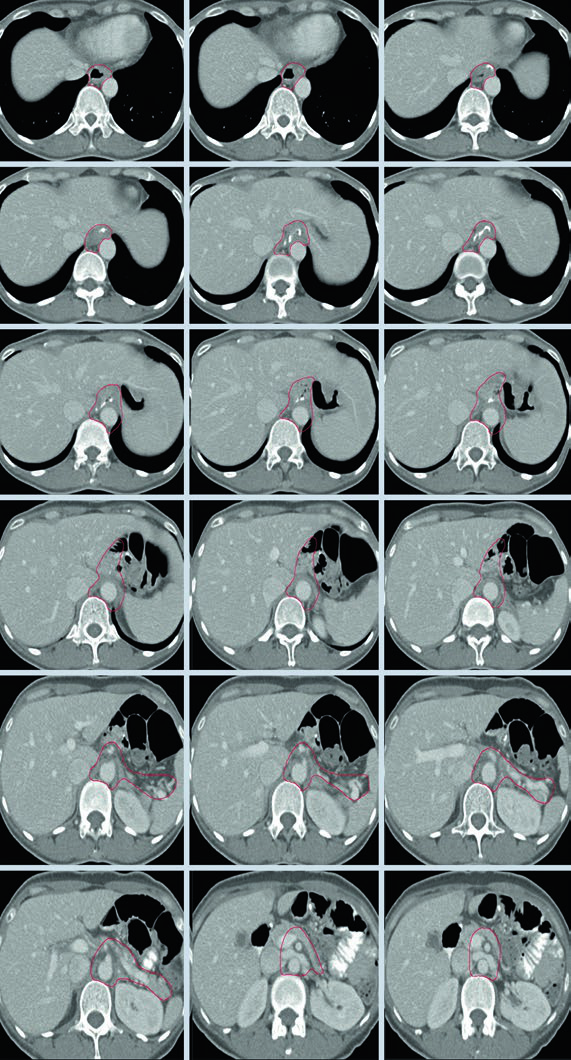
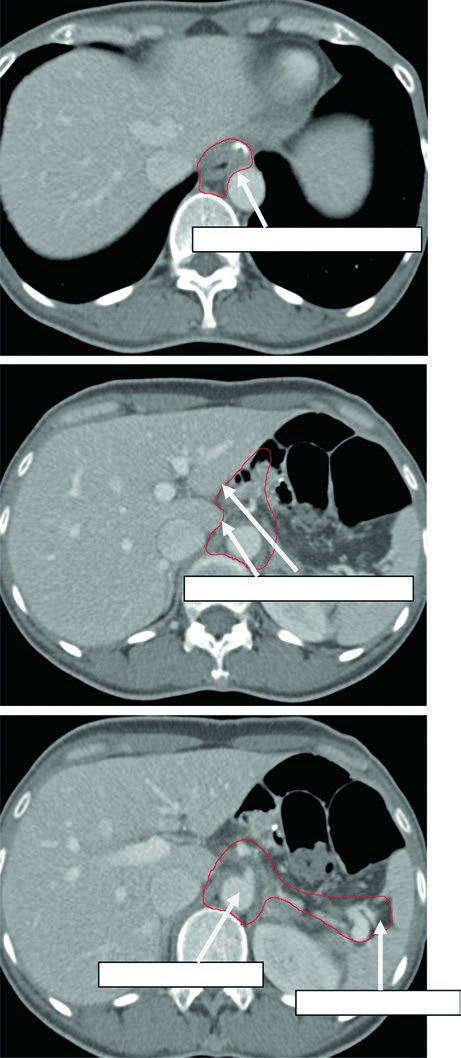
In this case, the CTV encompasses the esophagojejunal anastomosis, the hepatogastric ligament, the celiac artery, and the splenic hilum. Since this is a total gastrectomy for a node-positive cardia tumor, there is no gastric remnant to include, but nodal volumes must be comprehensive.
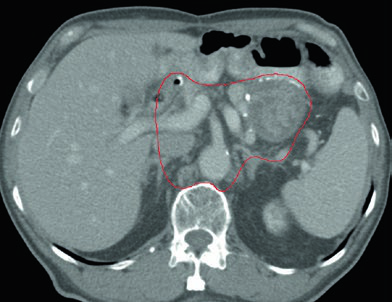
Case 2: T3N3M0 Body Adenocarcinoma — Distal Gastrectomy
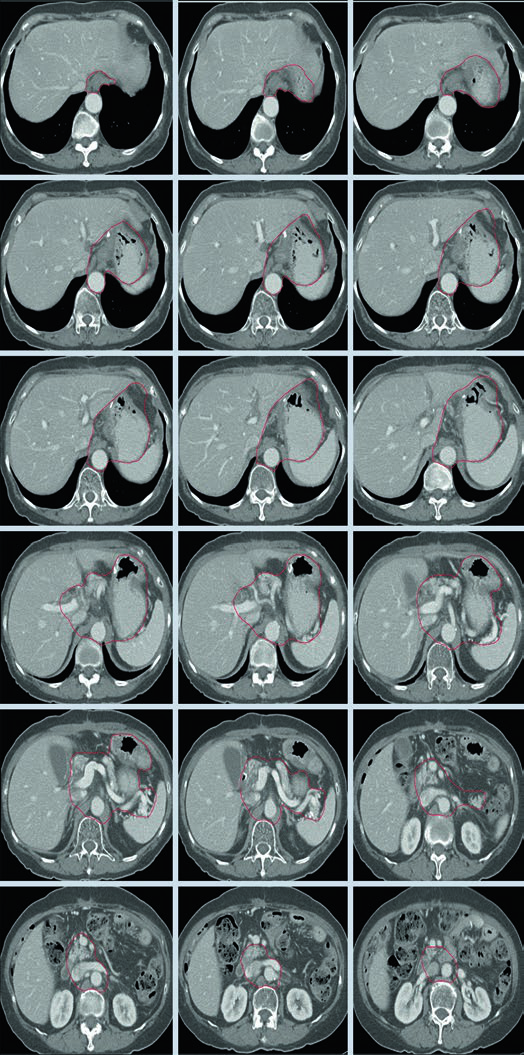
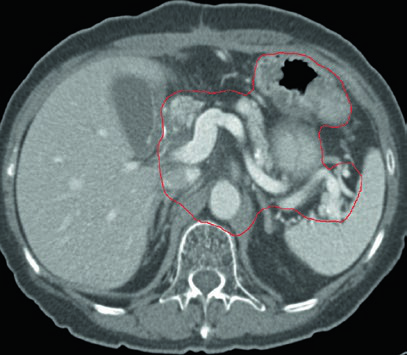

With T3N3 disease, the CTV is extensive: it includes the gastrojejunal anastomosis, the remnant stomach, the celiac artery, the splenic hilum, and the pancreatic tumor bed. This scenario requires careful attention to OAR dose constraints — particularly for the kidneys and liver — given the considerable treatment volume.
Case 3: T2N1M0 Antral/Pyloric Adenocarcinoma — Distal Gastrectomy
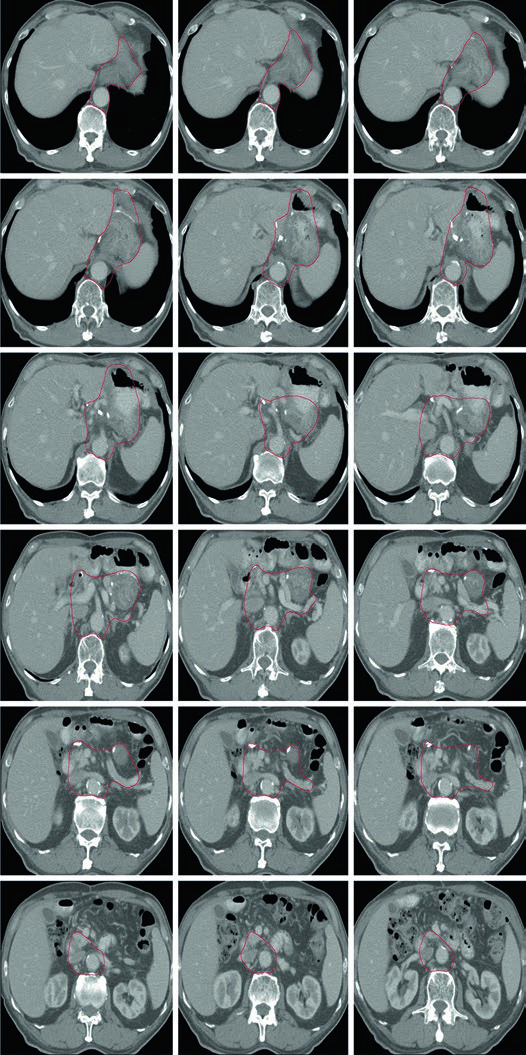
In antral/pyloric adenocarcinoma, the CTV covers the gastrojejunal anastomosis, remnant stomach, hepatogastric ligament, and duodenal stump. Splenic hilum coverage is optional here. The duodenal stump should preferably be covered in partial gastrectomies for distal/antral tumors but should not be included for proximal tumors treated with total gastrectomy.
Plan Assessment and Dose Constraints
In advanced cases, normal structure constraints — specifically for the spinal cord, kidneys, and liver — are typically prioritized over full tumor coverage. With 3D conformal technique, 100% of PTV45 should receive ≥42.75 Gy (95% of prescribed dose) per ICRU 62. With IMRT, 98% of PTV should receive ≥42.75 Gy per ICRU 83.
OAR Dose Constraints for Upper Abdominal Malignancies
| Organ at Risk | Dose Constraint | Endpoint | Rate (%) |
|---|---|---|---|
| Spinal cord | Dmax = 50 Gy | Myelopathy | 0.2 |
| Spinal cord | Dmax = 60 Gy | Myelopathy | 6 |
| Spinal cord | Dmax = 69 Gy | Myelopathy | 50 |
| Whole liver | Mean dose 30–32 Gy | Classical RILD | <5 |
| Whole liver | Mean dose <42 Gy | Classical RILD | <50 |
| Small intestine | V45 < 195 cc (entire peritoneal cavity) | Grade ≥3 acute toxicity | <10 |
| Heart | Mean dose <26 Gy (pericardium) | Pericarditis | <15 |
| Heart | V30 < 46% (pericardium) | Long-term cardiac mortality | <15 |
| Heart | V25 < 10% (whole heart) | Cardiac mortality | <1 |
| Bilateral kidneys | Mean dose <15–18 Gy | Clinically relevant renal dysfunction | <5 |
| Bilateral kidneys | Mean dose <28 Gy | Clinically relevant renal dysfunction | <50 |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 15.9)
Kidney sparing deserves particular attention in gastric cancer planning. For GEJ and cardia tumors, the plan aims to preserve two-thirds of the right kidney; for antral and pyloric tumors, two-thirds of the left kidney is spared. This asymmetry reflects the anatomy of tumor extension and the surgical bed.
General CTV Considerations for Adjuvant Therapy
The following table summarizes the general considerations guiding inclusion of the duodenal stump, anastomosis, para-aortic nodes, and paraesophageal nodes.
| Target Volume | Definition and Description |
|---|---|
| Duodenal stump | Preferably covered in partial gastrectomy for distal/antral tumors. Not to be covered in total gastrectomy for proximal/cardia tumors |
| Anastomosis | Gastrojejunal (partial gastrectomy for distal tumors) or esophagojejunal (total gastrectomy for proximal/GEJ tumors) — should be treated |
| Para-aortic nodes | Should be included for the entire length of the CTV |
| Paraesophageal nodes | 4 cm margin of the esophagus should be included in the CTV for GEJ tumors |
Source: Target Volume Delineation and Field Setup, 2nd Edition (Table 15.3)
The benefits of IMRT for adjuvant gastric radiotherapy have been suggested by multiple publications. When IMRT is used, both the tumor bed and subclinical target volumes — including lymphatic drainage regions — should be individually delineated. The PTV is generated by expanding the CTV with at least a 1 cm margin to account for organ motion and setup uncertainties.
Other articles in this series address techniques relevant to complex abdominal planning — such as esophageal cancer field setup and pancreatic cancer target delineation, which share similar challenges with organ motion management and renal dose sparing.


