

In This Article
General Planning and Simulation Principles
Radiation planning for esophageal cancer requires thorough knowledge of cervical, mediastinal, and abdominal anatomy, along with reliable motion compensation techniques. Both IMRT and 3D-CRT demand accurate delineation of target volumes, normal structures, and organs at risk (OARs), plus careful dose-volume histogram evaluation during planning.
At simulation, patients should ideally have their arms above the head to maximize beam arrangement options without beams traversing the upper extremities. For distal or gastroesophageal junction (GEJ) tumors, respiratory motion compensation is essential: 4D CT scanning, respiratory gating, or breath-hold techniques. Patients should remain nil per os (NPO) for at least 2–3 hours before simulation and each treatment session to limit daily anatomic variation from gastric and bowel gas.
For IMRT planning, intravenous contrast at simulation helps better delineate nodal fields. Contrast-enhanced planning CT improves distinction between lymph nodes and adjacent vascular structures — particularly important in the mediastinum.
For a broader perspective on target volume delineation across multiple anatomic sites, see our dedicated article on gastric cancer, which shares several abdominal planning principles with the distal esophagus.
Anatomic Subdivisions of the Esophagus
The esophagus begins in the neck at the lower border of the cricoid cartilage (anterior to the sixth cervical vertebra) and descends through the mediastinum, passing through the diaphragm into the abdomen. Using the standard 40 cm distance from the incisors to the GEJ, the subdivisions are defined as follows:
- Cervical esophagus: from the incisors to approximately 15–20 cm
- Upper thoracic (proximal) esophagus: from 18–20 cm to approximately 25 cm
- Lower thoracic (mid/distal) esophagus: from 25 cm to 30–32 cm
- Abdominal esophagus: from 30–32 cm to 40 cm
This anatomic subdivision directly guides CTV contouring and the selection of elective nodal stations. Tumors spanning multiple subdivisions should follow the contouring guidelines for all involved subsets.
Regardless of tumor location, the entire lungs must be contoured for adequate DVH analysis. For upper esophageal malignancies, the brachial plexus and larynx should be delineated. For lower esophageal tumors, the heart, liver, kidneys, stomach, and adjacent bowel must be included as OARs.
GTV, CTV, and PTV Delineation
The following target structures should be delineated: GTV (gross tumor volume), CTV (clinical target volume), and PTV (planning target volume). An ITV — the volume encompassing the internal motion of the GTV observed on 4D CT — is routinely defined at institutional level. The ITV is expanded to a CTV, then to a PTV.
Physicians should delineate the GTV with reference to CT and PET imaging, as well as findings on upper endoscopy and endoscopic ultrasound (EUS). EUS is particularly valuable for staging tumor invasion depth and classifying small periesophageal lymph nodes that are difficult to assess by CT or PET alone. If the tumor is superior to the carina, bronchoscopy is recommended to rule out tracheoesophageal fistula, which may delay radiotherapy.
Standard ITV-to-CTV expansions are 1 cm radially (to encompass periesophageal lymph nodes) and 3–4 cm in the superior-inferior direction (oriented along the esophageal mucosa) to account for submucosal spread and possible skip lesions. The CTV expansion can be limited to 0.5 cm in areas overlapping the heart and uninvolved liver, assuming appropriate motion management.
For distal and GEJ tumors, a 4 cm caudal margin would include large volumes of stomach or abdominal viscera. The recommendation is only 2 cm margin to CTV along clinically uninvolved gastric mucosa — unless treating with preoperative-intent doses (≤4500 cGy), where a 4 cm or greater gastric margin may be appropriate, particularly for tumors with significant gastric extension.
Uninvolved vertebral bodies and kidneys are excluded from the CTV. For involved lymph nodes, a GTV-to-CTV margin of 0.5–1.0 cm is used. If grossly involved periesophageal nodes are present, the CTV should cover at least 1 cm cephalad to them. The recommended CTV-to-PTV expansion is 0.5 cm.
Nodal Coverage by Tumor Location
Regional lymph node inclusion in the CTV depends on the location of the primary tumor within the esophagus. Getting this right is critical — under-coverage risks regional failure, while over-coverage increases toxicity needlessly.
Cervical and proximal thoracic esophagus: bilateral supraclavicular nodal basins are included. The cranial boundary is the lower edge of the cricoid cartilage; the anterior, posterior, and lateral boundaries are defined by the sternocleidomastoid muscle. For proximal thoracic tumors, mediastinal lymph nodes are included beyond the periesophageal nodes — encompassing the entire trachea, levels 2 and 4, extending toward the sternum and clavicular heads to cover level 3.
Distal thoracic esophagus: the CTV should include the celiac nodes, bounded on the right by the lateral aspect of T12, on the left 0.5–1 cm beyond the lateral aspect of the aorta, posteriorly by the vertebral bodies, and anteriorly by the pancreas. It is not necessary to include superior mediastinal nodal stations electively, beyond overlap with the cranial expansions.
GEJ tumors: the CTV should include para-aortic and gastrohepatic ligament nodes, in a volume bounded by the liver on the right and the stomach on the left. For tumors also requiring abdominal planning, see our article on pancreatic cancer, which discusses celiac axis anatomy and motion management in detail.
Siewert–Stein Classification for GEJ Tumors
When GEJ tumors significantly overlap the gastric cardia, the question of esophageal versus gastric origin becomes ambiguous. The Siewert–Stein classification addresses this by defining GEJ tumors according to their epicenter relative to the junction:
- Type I: epicenter 1–5 cm above the junction
- Type II: epicenter from 1 cm proximal to 2 cm distal to the junction
- Type III: epicenter 2–5 cm below the junction
A reasonable cutoff for esophageal cancer is Siewert type II. The eighth edition AJCC staging system now defines esophageal tumors as those whose epicenter extends no more than 2 cm into the gastric cardia. For Siewert type II tumors, some or all of the splenic hilum and greater curvature nodal region may be included in the CTV.
Based on prevailing guidelines for gastric cancers, diagnostic laparoscopy, J-tube placement, preoperative or postoperative chemoradiation can be considered. For more detail on gastric planning, see our dedicated article on gastric cancer.
Contouring Recommendations by Esophageal Subdivision
The following table summarizes the recommended margins, elective nodal coverage, and dose prescriptions for each anatomic subdivision of the esophagus. These data form the backbone of treatment planning — keep them accessible during contouring.
| Subdivision | Definition | ITV→CTV Margin | CTV→PTV Margin | Elective Nodal Coverage | Dose |
|---|---|---|---|---|---|
| Cervical | Incisors to ~15–20 cm | 3 cm sup/inf (mucosa), 1 cm radial | 0.5 cm | Periesophageal, supraclavicular, ± anterior mediastinal | 50.4 Gy at 1.8 Gy/fx, boost to 60–70 Gy for SCC |
| Upper thoracic | 18–20 cm to ~25 cm | 3 cm sup/inf (mucosa), 1 cm radial | 0.5 cm | Periesophageal, supraclavicular, ± anterior mediastinal | 50.4 Gy at 1.8 Gy/fx |
| Lower thoracic | 25 cm to ~37 cm | 3 cm sup/inf (mucosa), 1 cm radial | 0.5 cm | Periesophageal | 50.4 Gy (definitive); 41.4–50.4 Gy (preoperative) |
| Abdominal (GEJ) | ~37 to 42 cm | 3 cm sup (esoph. mucosa) + 1–2 cm inf (gastric mucosa); ≥4 cm gastric if preop ≤4500 cGy | 0.5 cm | Periesophageal, gastrohepatic ligament (paracardiac + left gastric), celiac axis, ± splenic hilum | 50.4 Gy (definitive); 41.4–50.4 Gy (preoperative) |
Source: Target Volume Delineation and Field Setup: A Practical Guide for Conformal and Intensity-Modulated Radiation Therapy, 2nd Edition (Table 14.1)
Illustrated Clinical Cases
The following cases, drawn directly from the textbook, illustrate the practical application of these guidelines in real-world scenarios. Each case demonstrates how to integrate PET, endoscopy, and EUS findings into volume contouring.
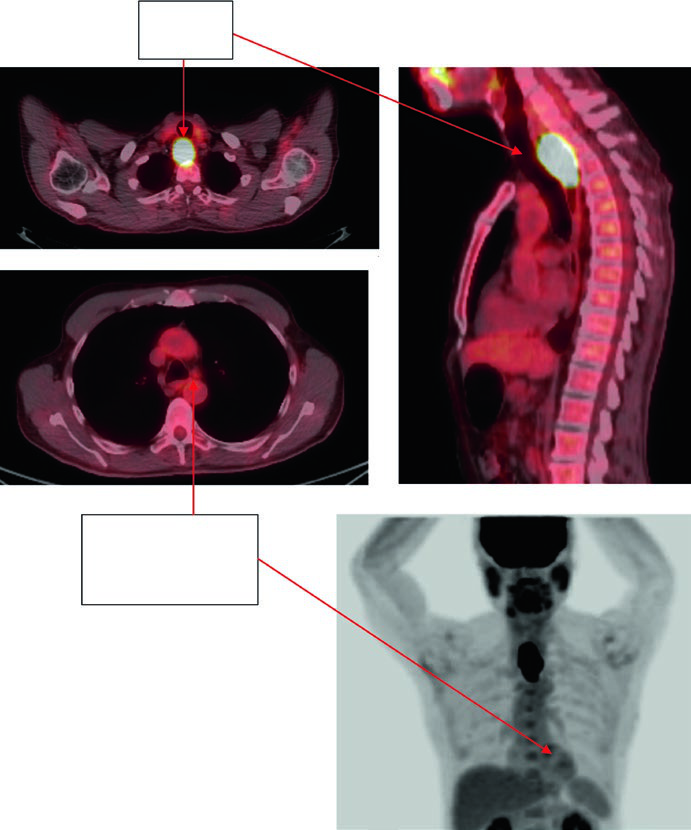
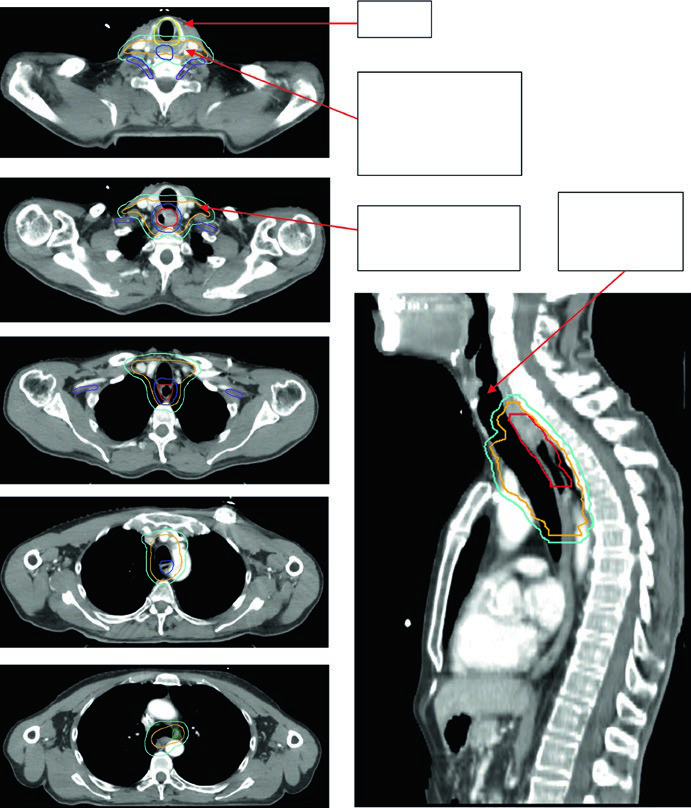
Case 1: Cervical/Upper Thoracic SCC — 69-Year-Old
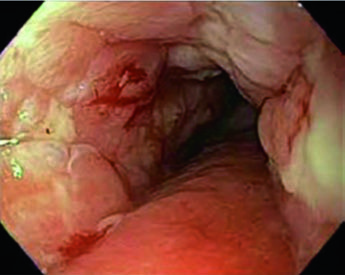
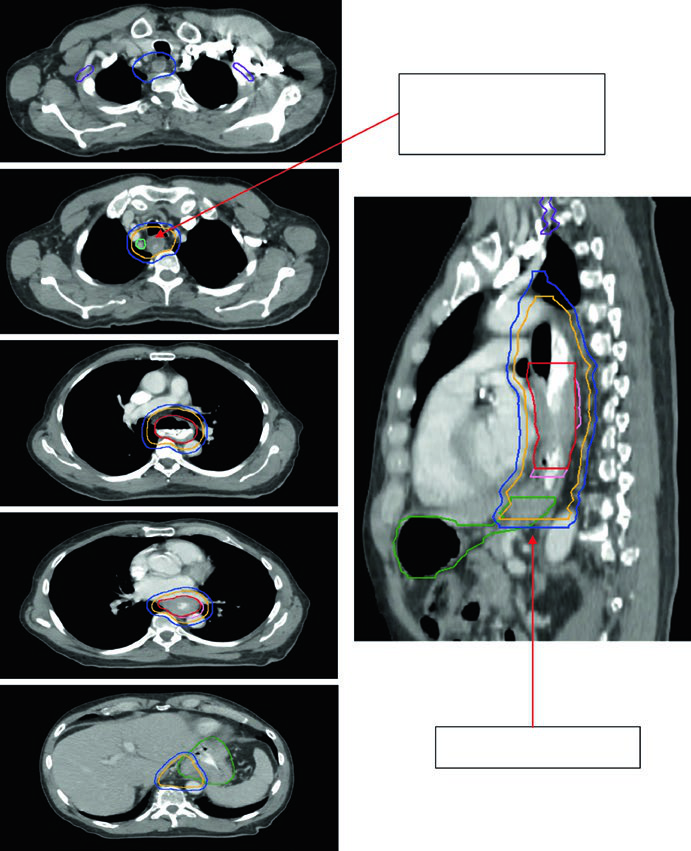
A 69-year-old patient with SCC of the cervical/upper thoracic esophagus. PET-CT revealed FDG-avid primary and mildly avid paratracheal lymph nodes. EGD showed an ulcerating submucosal mass 15–23 cm from the incisors. Delineated volumes included: brachial plexus (purple), larynx (yellow), esophageal GTV (red), nodal GTV (green), CTV (orange), PTV 54 Gy (cyan), and PTV 60 Gy (dark blue). The superior border of the supraclavicular field was placed at the inferior border of the cricoid cartilage, with bilateral elective SCV nodal coverage.
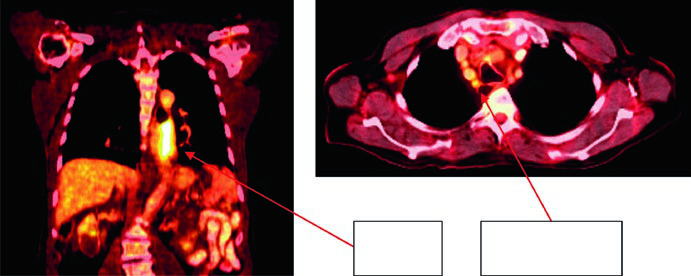
Case 2: Lower Thoracic Adenocarcinoma — 81-Year-Old, uT3N1
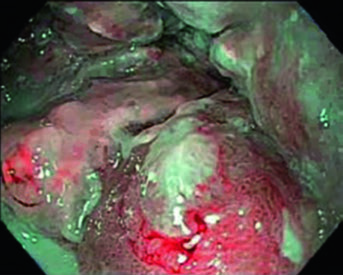
An 81-year-old patient with lower thoracic esophageal adenocarcinoma uT3N1. PET showed primary uptake and level 4R paratracheal lymph node. Endoscopy revealed a partially obstructing circumferential adenocarcinoma 31–35 cm from the incisors. EUS confirmed T3 primary disease with suspicious level 4R node. Contours applied a 0.5 cm GTV-to-CTV margin for the 4R node and 3–4 cm inferior coverage. Volumes: brachial plexus (purple), stomach (dark green), esophageal GTV (red), ITV (pink), nodal GTV (light green), CTV (orange), PTV 50.4 Gy (dark blue).
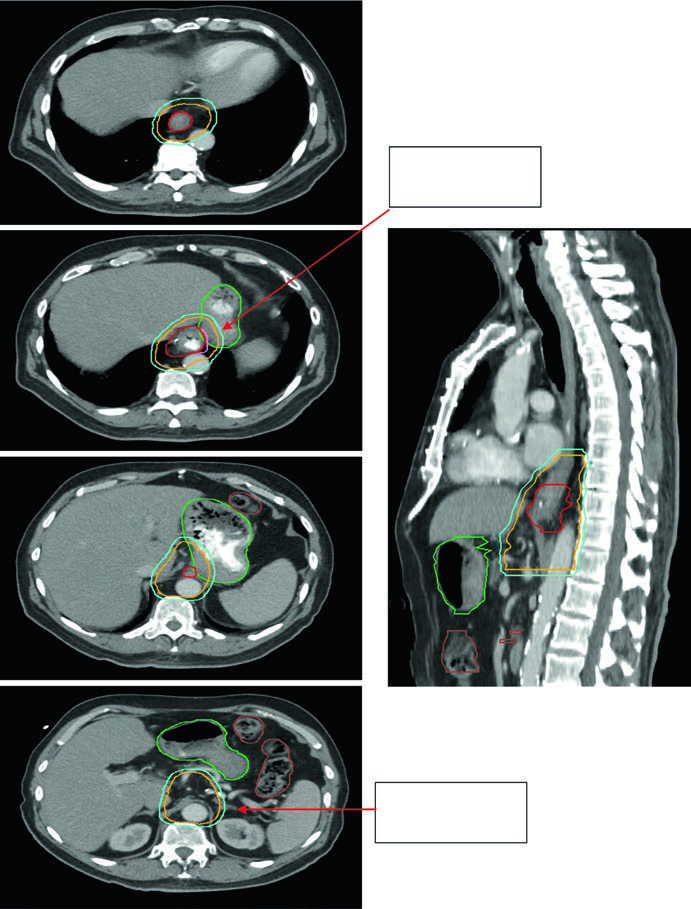
Case 3: GEJ Adenocarcinoma — 75-Year-Old, uT3N0
A 75-year-old patient with GEJ adenocarcinoma uT3N0. Contours demonstrate CTV extension into the proximal stomach with coverage to the celiac axis. Delineated volumes: stomach (dark green), large bowel (brown), esophageal GTV (red), CTV (orange), PTV 50.4 Gy (cyan). Celiac axis coverage is mandatory for distal and GEJ tumors.
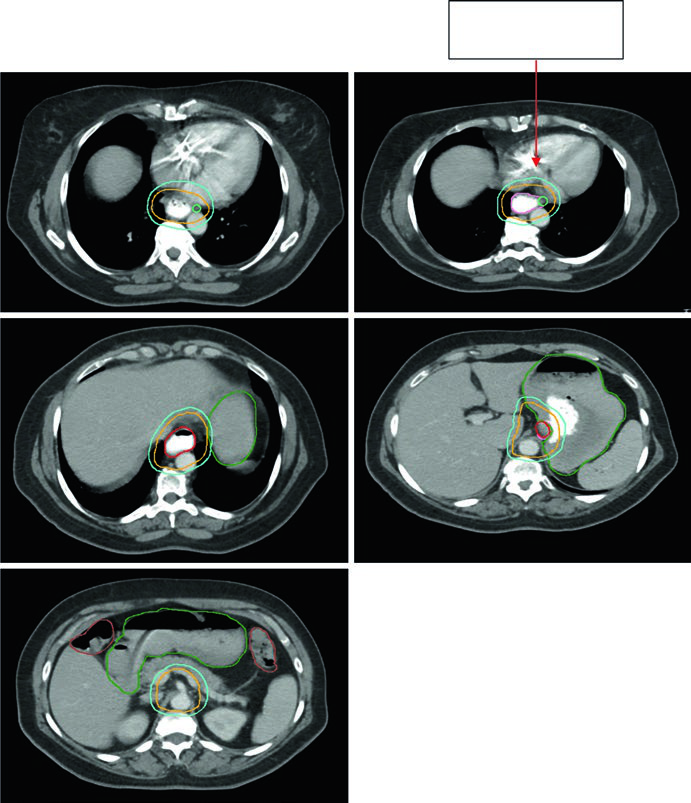
Case 4: GEJ Adenocarcinoma — 59-Year-Old, uT3N2
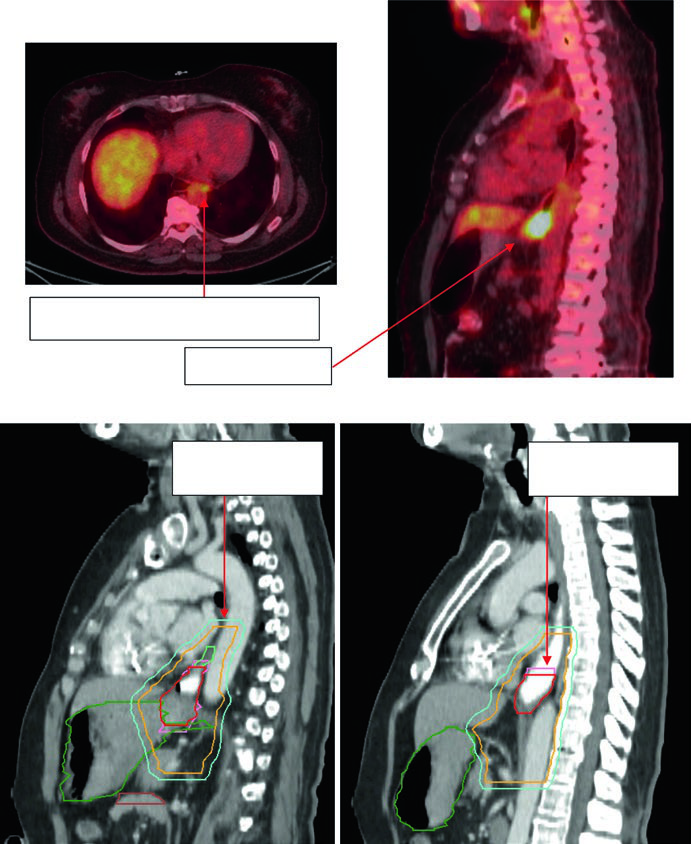
A 59-year-old patient with GEJ adenocarcinoma uT3N2. PET showed FDG-avid paraesophageal nodes and primary located 36–40 cm from the incisors. The sagittal planning CT shows the ITV reflecting GTV movement, with CTV covering 3–4 cm above the ITV. Volumes: stomach/duodenum (dark green), nodal GTV (light green), esophageal GTV (red), ITV (pink), CTV (orange), PTV 50.4 Gy (cyan). Paraesophageal lymph nodes were included in the treatment field.
For similar principles applied to other thoracic and abdominal sites, see our article on lung cancer and the discussion on rectal cancer, covering respiratory motion management and pelvic delineation respectively.


