

This debate usually appears too late. In many services, it only enters the conversation when a plan calculated in AAA does not match a case recalculated in Acuros XB, when a Monte Carlo of RayStation makes a difference in bone, or when someone tries to add imported distributions without being sure about the magnitude that each engine is reporting.
This is where simplification takes its toll. Treat dose to water as tradition and dose to medium like modernity doesn’t solve anything. The useful question is another: what physical response is TPS delivering in that voxel and what changes when that voxel stops behaving like almost homogeneous water.
Dose to medium and dose to water can be very close together in various soft tissues. But they cease to be interchangeable precisely in scenarios in which the algorithm begins to see real material: bone, implant, strong heterogeneity and comparison between engines from different families.
In this Article
- 1. Where does this difference arise
- 2. What does dose to medium mean
- 3. What dose to water means
- 4. Where the difference is usually small
- 5. Where the difference is no longer small
- 6. Why the bone is so important in this discussion
- 7. What does the Acuros figure help you see
- 8. As this appears in trading algorithms other than
- 9. The most common methodological error
- 10. Detectors, measurements and the illusion of automatic equivalence
- 11. Does this change the clinical decision?
- 12. A coherent institutional policy avoids half the confusion
- 13. Which convention makes the most sense?
- 14. What a service should do in practice
- 15. The right question when closing a plan
Where does this difference arise
The distinction appears more clearly when an algorithm starts to treat the patient as a set of real materials, and not just as water scaled by density.
In Acuros XB, for example, the calculation chain solves for electron fluence in the real medium and then converts this information into dose. The Eclipse guide itself summarizes the final stage as follows:
The decisive point is which properties are used in this conversion:
- if the algorithm uses the local material properties, it reports dose to medium;
- if the water response is used, it reports dose to water.
This difference is physical, not semantic. In both cases, creep was obtained for transport in the real environment. What changes is the “receptor” used to transform this fluency into a reportable dose.
What does dose to medium mean
Dose to medium means, in practical terms, the energy deposited per unit of mass in the voxel material itself. If the voxel represents bone, the answer is bone. If it represents lung, the answer is that of the lung. If it represents muscle, the answer is that of the muscle.
This approach tends to sound more natural when the algorithm already works with explicit mapping material, as in Acuros XB. In this context, reporting dose to medium is consistent with the logic of the calculation itself: the transport was resolved in the real environment and the final conversion also respects the real environment.
What dose to water means
Dose to water mean using the water response to convert the calculated fluence. In many cases, this functions as a way of maintaining historical comparability with a dosimetric tradition built around water as a reference.
The important point is that dose to water does not imply that transport has been resolved in water. In modern algorithms, it is perfectly possible to transport in the real environment and, in the end, report dose as if a small volume of water were inserted in that fluence field.
This detail is central because it explains why the difference between the two modes grows in materials whose behavior is further away from that of water.
Where the difference is usually small
The local documentation of the RayStation is especially useful here. The system warns that, when transport is resolved in the real environment, the differences between dose to water and dose to medium for photons are usually small in tissues other than bone, typically in the range of 1–2%.
This observation is important because it prevents frequent exaggeration: transforming every convention difference into a large clinical effect. In most soft tissues, the discrepancy may in fact be modest.
But “modest” does not mean “always irrelevant”. In radiotherapy, a small effect may cease to be small depending on:
- local gradient;
- analyzed volume;
- clinical objective;
- use of data in inter-algorithmic comparison;
- decision on re-irradiation or background dose.
Where the difference is no longer small
The same warning as RayStation It is clear that the discrepancy can become relatively large in bone, reaching something on the order of 10%, and also in other high atomic number materials.
Eclipse reinforces this line when discussing the conversion of fluence to dose in Acuros XB. The guide highlights that the effect is most significant:
- in high-density non-biological materials such as aluminum, titanium and steel;
- in bone, among biological materials.
This part is fundamental because it shows that the difference between dose to medium and dose to water does not manifest itself uniformly. It focuses precisely on where water stops being a good implicit substitute for the real material.
Why the bone is so important in this discussion
The bone is usually the point at which the conversation stops being theoretical. It is biologically relevant, appears in several treated sites and already has properties sufficiently different from water to expose the convention used by the algorithm.
Handbook of Radiotherapy Physics reinforces this by commenting on comparisons between AAA and Acuros XB. The text highlights that, in studies comparing the two reporting options in the context of materials such as bone and lung, the significant difference appears mainly in bone and that the dose to medium option was recommended by the authors in one of the benchmarks mentioned.
This observation is valuable because it puts the question back in the right place. The debate is not “which option seems more elegant”, but “which magnitude is more coherent with physics and more useful for the clinical interpretation of this case?”.
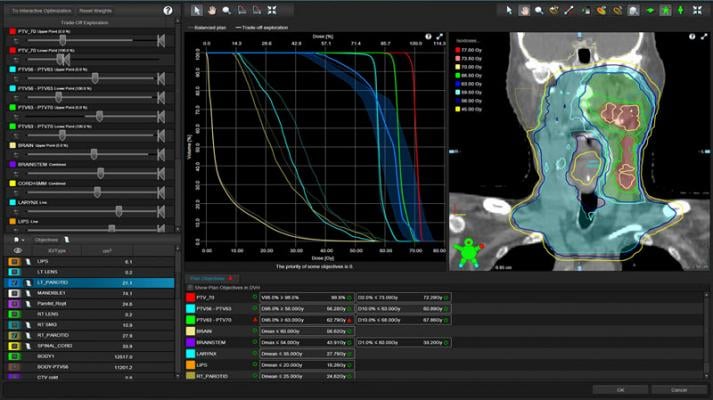
What does the Acuros figure help you see
The figure taken from Varian’s guide on energy deposition ratios and collisional stopping power ratios is particularly good for this topic:
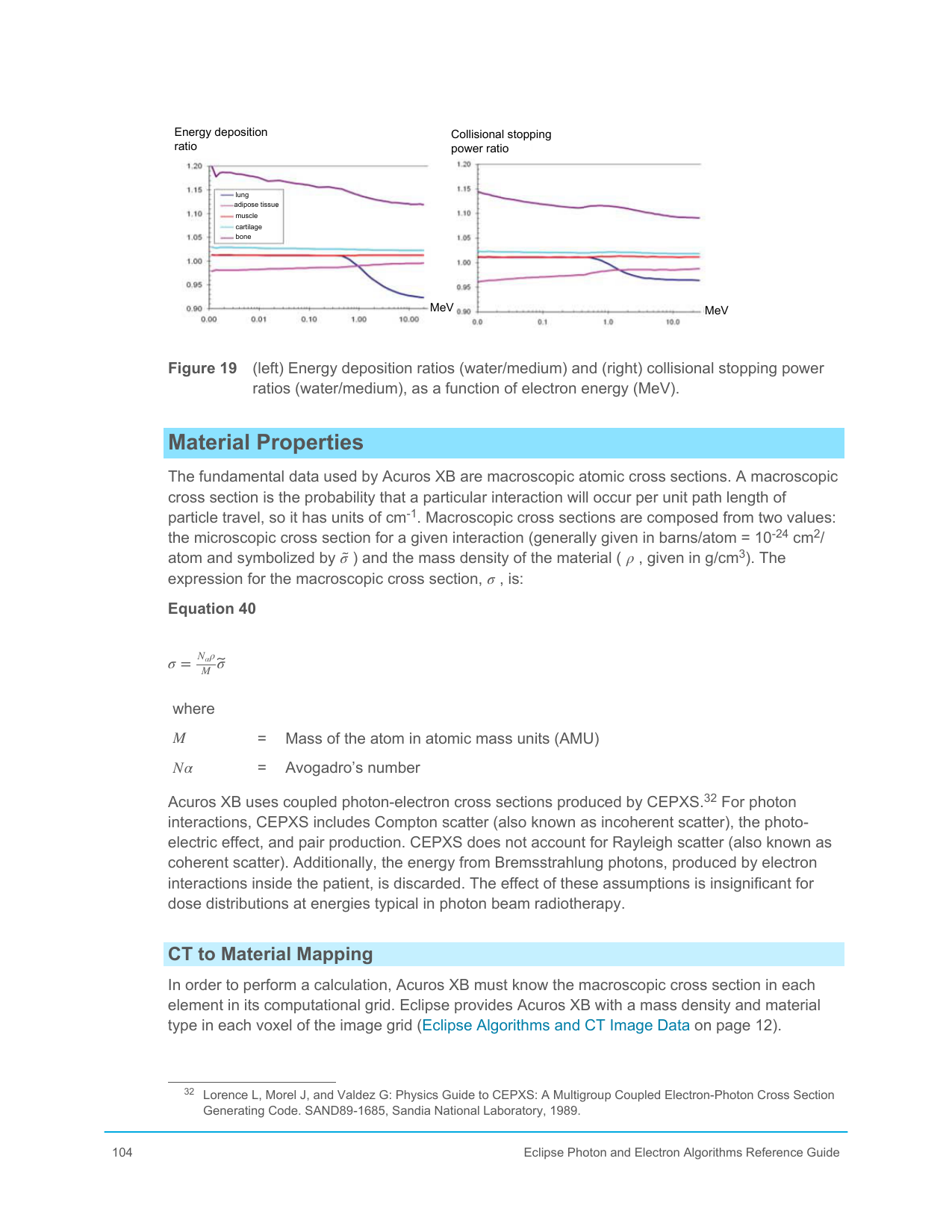
It shows that:
- the ratio between dose to water and dose to medium calculated by energy deposition;
- and the reason based on stopping powers,
do not behave identically across all materials and energies.
This point is crucial. When someone compares dose numbers between different algorithms as if they were directly equivalent, they may be comparing physical objects that are close but not identical.
As this appears in trading algorithms other than
Acuros XB
In Acuros XB, the user can explicitly choose dose to medium or dose to water. As the algorithm already works with materials and mass density, this choice appears as a visible part of the final dose interpretation.
RayStation
In RayStation, the situation is even more didactic because the system itself coexists with engines that follow different conventions. The local notice says:
- o photon collapsed cone computes dose for water with transport in water of variable density;
- o photon Monte Carlo reports dose for medium with transport in medium.
In other words: the service can, within the same TPS, deal with distributions that arise from different conventions.
Older or more simplified algorithms
In older or less material-explicit engines, the discussion is sometimes hidden because the construction of the algorithm itself already presupposes scaled water or equivalents. This doesn’t eliminate the question; it just makes it less visible.
The most common methodological error
The most common error in this area is not choosing “the wrong convention”. It’s mixing magnitudes without realizing it.
This happens in several contexts:
- comparing plans between different algorithms;
- use of background dose;
- dose sum;
- co-optimization;
- fallback between engines;
- comparison with doses imported from external systems.
RayStation is very explicit in warning that the dose convention of imported distributions may be unknown and that any combination should be treated with caution when the case is sensitive to high Z.
This warning should be read as a general rule of modern clinical practice. The problem is not “mixing software”. The problem is mixing physical quantities without clearly declaring what each one represents.
Detectors, measurements and the illusion of automatic equivalence
Varian’s guide makes a very important observation when commenting dose to water on Acuros XB: in non-aqueous materials, the small volume of equivalent water that would receive that dose can be much smaller than the calculation voxel or a detector used in experimental measurement.
This detail is deeply clinical. Often the “algorithm versus measurement” comparison is treated as if both sides are describing exactly the same physical object. They aren’t always.
In practical terms:
- a detector in water or calibrated in water-equivalent conditions carries a specific dosimetric tradition;
- a bone voxel in a material-explicit algorithm describes another physical context;
- direct comparison between the two requires interpretation, not just subtraction.
This is precisely why Acuros XB recommends, in certain cases, explicitly modeling a small volume of water representing the detector.
Does this change the clinical decision?
The serious answer is: it depends on the case, but sometimes it does change.
In homogeneous soft tissues, the difference may not alter conduct. In bone, implants and dense materials, it may alter the local dose reading. And even when it doesn’t change the final clinical decision, it can change the interpretation of:
- why two algorithms diverge;
- whether a discrepancy is physical or methodological;
- whether an objective is actually being met;
- how much of the difference belongs to the algorithm and how much belongs to the reporting convention.
This last point is particularly important in auditing and in comparisons between services. Sometimes two groups appear to disagree about the algorithm, when in fact they are discussing differently reported quantities.
A coherent institutional policy avoids half the confusion
Few people like to formalize this type of decision, but a simple institutional policy usually avoids a lot of noise. This policy should declare:
- which convention will be prioritized by default in each TPS;
- in which contexts the other convention will be maintained or used for comparison;
- how the service will handle dose sum and background dose;
- how to document imported distributions whose convention is not obvious;
- in which scenarios the team should interpret bone and high Z with enhanced caution.
Without this type of institutional agreement, the risk is that the issue will only reappear in moments of conflict, when two physicists are already looking at different numbers and calling them both a “dose”.
Which convention makes the most sense?
There is no universally neutral response, but there is a more technically conscious response.
If the algorithm solves transport in a real environment and the objective is to maintain local physical coherence, dose to medium makes a lot of sense. This is why it is usually defended in discussions linked to material-explicit engines.
If the central objective is comparability with certain dosimetric traditions and with a historical language strongly anchored in water, dose to water continues to have appeal.
The problem begins when the choice is made out of habit and not out of understanding. The chosen convention needs to be known by the physicist, the service and, ideally, be clear whenever there is a comparison between engines.
What a service should do in practice
A mature methodological stance includes at least five precautions:
- knowing which convention each engine is using;
- document the institutionally adopted convention in relevant scenarios;
- avoid comparing different engine plans as if the magnitude were automatically the same;
- pay special attention to bone, implants and high Z;
- materials distinguish convention difference from algorithmic transport difference.
This is not bureaucracy. It is the only way to prevent a legitimate physical detail from being read as a non-existent clinical error or, worse, from a real difference being disguised as mere convention.
The right question when closing a plan
Perhaps the most useful way to close this topic is with an operational question:
when I read this dose value, am I reading the response of the real medium or the response of the water in that creep field?
If the team knows how to answer this immediately, much of the confusion disappears. If you don’t know, comparing different engines will continue to seem more mysterious than it really is.


