

What the study reveals
Adnexal lesions scored as O-RADS 4 or O-RADS 5 on pelvic ultrasound should function as alarm signals — categories that, in theory, indicate high probability of malignancy. A new study published in Radiology pours cold water on that assumption: 62% of lesions classified as O-RADS 4 or 5 turned out to be benign. The finding pressures the positive predictive value (PPV) of the upper categories of the ACR system and reopens the debate on ovarian ultrasound screening.
O-RADS US (Ovarian-Adnexal Reporting and Data System for ultrasound) was proposed by ACR to standardize reports and stratify risk in adnexal lesions. Categories from 1 to 5 map increasing probability of malignancy; in practice, lesions scored 4 and 5 should trigger complementary imaging (MRI, CEUS) or surgical referral. When 62% of that population is confirmed benign on histology, the bill — clinical, surgical, and emotional — is steep for the patient.
Methodology and sample
The multicenter, retrospective study analyzed 219 ovarian or adnexal lesions in 203 patients (median age 47) who had pelvic ultrasound. Of the 219 lesions, 133 were initially classified as O-RADS US 4 and 86 as O-RADS US 5. After follow-up and histopathological analysis:
- 135 of 219 (62%) were benign overall.
- 84% of O-RADS 4 (112/133) were benign.
- 27% of O-RADS 5 (23/86) were benign.
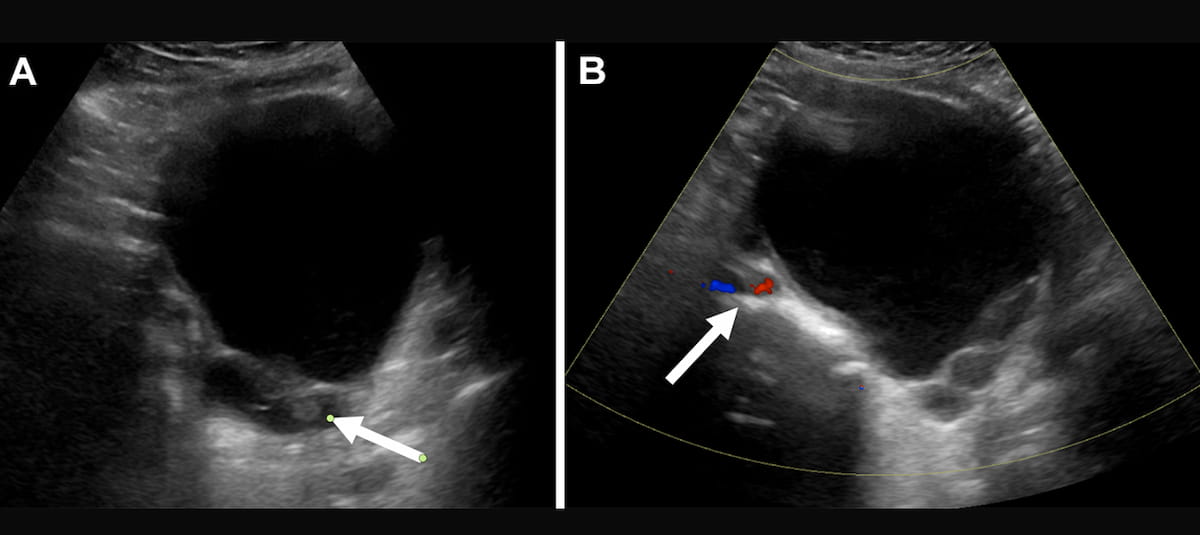
The authors, led by radiologist Priyanka Jha (Stanford), report that cystadenomas and cystadenofibromas accounted for 46% of the benign lesions classified as O-RADS 4 or 5. These tumors may show papillary projections and mural nodules — findings classically signaling malignancy.
Why so many false positives?
Two imaging findings dominated misclassified cases:
- Solid component in 71% of misclassified benign lesions.
- Multilocularity in 45% of cases.
“Solid components and multilocularity in benign lesions can mimic malignancy and lead to scoring as O-RADS US 4 or 5, ultimately driving down the positive predictive value of these categories,” the authors write. The simple read: the features used to push a lesion up the risk ladder are not discriminative enough when it comes to fibromatous cystadenoma or tumors with dense fibrous tissue.
Three key takeaways for practice
The study leaves clear operational lessons for the clinical radiologist:
- High false-positive rate: a substantial share of “high-risk” lesions on ultrasound are benign — 84% of O-RADS 4 and 27% of O-RADS 5. This drops PPV and limits the reliability of categorization for malignancy stratification.
- Main mimickers: solid component (71%) and multilocularity (45%) lead the diagnostic confusion.
- Adjunct imaging and technique refinement: dynamic assessment (solid component movement, acoustic shadowing) and follow-up with CEUS or MRI can improve differentiation between true solid tissue and mimickers.
Implications for management
The paper suggests practical paths to cut false positives. Cine clips during acquisition can reveal mobility of the solid component (suggesting debris or organized clot rather than tumor) and acoustic shadows that point to calcifications in cystadenofibroma. CEUS and MRI add information: both can show enhancement in genuinely vascularized tissue, with time-intensity curves useful to tell benign from malignant lesions apart.
For services running high volumes of gynecologic ultrasound, this discussion overlaps with that of a CT nomogram for advanced ovarian cancer management and the expansion of oncology platforms such as the MIM ComboTherapy GYN. Gynecologic imaging is in rapid transition: standardized reporting, multimodal imaging, and AI algorithms are all being tested to refine risk stratification.
Limitations acknowledged by the authors
The Stanford group itself lists important limitations:
- Patients with initial benign assessments were excluded, which may bias the PPV estimate downward.
- There was no central expert review of images; each case kept the original interpretation.
- Exams were performed by technologists without specific gynecologic imaging training in part of the cases — a factor that may have increased acquisition variability.
These limitations matter: services with radiologists dedicated to female pelvic imaging and sonographers trained in gynecologic ultrasound likely achieve PPVs higher than those reported. Still, the lesson stands — ultrasound alone is not enough to confirm malignancy in adnexal lesions.
What to expect
Recent literature is moving toward protocols that combine dynamic US, CEUS, and MRI in selected cases, with AI algorithms emerging to support classification. The next O-RADS US revision is expected to explicitly fold in these findings — possibly recalibrating criteria for solid component and multilocularity, or subdividing categories 4 and 5 based on extra features. Until then, the experienced radiologist remains the most reliable filter against unnecessary surgery.
A practical implication often missed in the discussion is the burden on follow-up workflows. Every O-RADS 4/5 ultrasound that ends up benign still generates downstream MRI orders, multidisciplinary meetings, and patient anxiety in the interval. Departments that already operate at MRI capacity may not absorb a doubling of complementary imaging requests, which makes the case for in-house triage protocols — possibly with AI-assisted lesion scoring — even stronger.
Finally, the study is a reminder that risk-stratification systems live and die by the data they were calibrated on. O-RADS US was built on cohorts that may not represent the full spectrum of fibromatous adnexal disease seen in routine practice. A field-wide recalibration, ideally using prospective multicenter data with central expert review, is overdue.
Source: Diagnostic Imaging — Over 60 Percent of O-RADS 4 and 5 Lesions on Ultrasound Are Benign


