Choosing radiotherapy equipment based on solid technical specifications is the kind of decision that echoes for years: procurement, commissioning, training, daily operation, and the ability to keep treatments safe, consistent, and auditable.
This complete guide turns the reference document into a practical storyline: what sits inside the scope, which equipment categories matter, how equipment packages map to health-system capacity, and why a needs assessment should be treated as part of technology management, not as a one-off shopping list.
Chapter 1: Technical Specifications for Radiotherapy Equipment
Chapter 1 makes a clear point: radiotherapy relies on complex electromechanical devices, radiation sources, and software, and the technical specification is what turns that complexity into safer selection, procurement, training, and clinical use.
The context described in the publication is tied to global health-technology and cancer-control priorities. After the adoption of WHA resolutions on health technologies and cancer prevention/control, the World Health Organization published, in 2017, Lists of priority medical devices for cancer management to support prioritization and incorporation into health systems. Radiotherapy is positioned as integral in both curative and palliative care.
One line in the background section is worth keeping in mind when prioritizing investment: radiotherapy has the potential to benefit about 50% of cancer patients during the course of their disease. For cervical cancer, the text highlights a particularly strong population-level benefit of evidence-based radiotherapy, describing a 5-year overall survival benefit of 18% and 5-year local control of 33%. Improving access to radiotherapy is also described as a strategic action aligned with a 90% treatment target in the global strategy toward eliminating cervical cancer as a public health problem.
Operationally, that framing matters. It pushes the conversation beyond “buy a machine” and into “build a service”: equipment, standards, safety measures, quality assurance, and the organizational capacity to run the program reliably.
The publication is designed to support exactly that decision space. It is written for a multidisciplinary committee that includes clinical radiation oncologists, medical physicists, and biomedical engineers, but also information technology, financial, and planning officers. The goal is not to promote brands, but to provide specifications for commonly used radiotherapy equipment and help stakeholders select technology that enables clinical procedures to be performed safely, securely, and with good quality.
The document also states that it builds on earlier radiotherapy technical specifications (including an IAEA publication from 2008) and expands the view to include imaging, planning software, information management software, and ancillary equipment required to support the service.
How to Use This Guide (and the Follow-Up Articles)
The material is organized as a working blueprint: one chapter clarifies scope and core equipment; another defines equipment packages linked to health-system capacity and a needs-assessment method; subsequent chapters describe EBRT and brachytherapy items in a repeatable structure (description, IEC/ISO standards, sample specification, radiation safety/protection, and QA recommendations); and later chapters address service establishment and emerging technologies. If you want the full map of that structure before diving into item-by-item detail, see the dedicated article on how the publication is organized and how to apply it in practice.
Scope, Exclusions, and Intended Audience (Still Chapter 1)
Chapter 1 defines a scope that targets the core of cancer radiotherapy: treatment equipment, associated imaging, software (planning and information management), and ancillary devices that underpin safety and quality.
The text connects equipment planning to six reference cancers (breast, cervical, colorectal, leukaemia, lung, and prostate). It notes that these cancers can be treated with external beam radiotherapy (EBRT) with or without brachytherapy, together with associated imaging and treatment planning services. There is also a specific mention that cervical and prostate cancers are amenable to a high-dose-rate (HDR) brachytherapy intervention, reinforcing why a comprehensive service cannot treat brachytherapy as “optional.”
Equally important are the exclusions. Cancer treatments involving unsealed radioactive sources (for example, iodine-131 treatments for thyroid cancer) are not covered. Less frequently used modalities such as neutrons, protons, and light ions (for example, carbon ions) are not included in the technical-specification set. The publication acknowledges emerging evidence of improved organ-at-risk sparing with proton therapy for specific indications (including paediatric cancers), but it points to the lack of cost-effectiveness evidence and potential advantage in low- and middle-income country settings; emerging technologies are reviewed separately in the chapter on recent and emerging techniques.
Finally, the intended audience is broad by design. The final selection depends on national cancer control plans, infrastructure, workforce availability (radiation oncologists, medical physicists, radiation therapists, and biomedical/clinical engineers), budgets, and in some contexts whether radiotherapy is covered by national medical insurance or equivalent mechanisms. That is why the publication speaks not only to clinical and physics teams, but also to administrators, procurement officers, logisticians, regulatory authorities, and global procurement agencies. Manufacturers are explicitly part of the picture, with an expectation of compliance to support safe, high-quality, and affordable equipment appropriate for limited-resource settings.
For planning teams, the practical implication is to treat equipment selection as a shared responsibility. Clinical goals, safety constraints, staffing realities, IT integration, and budget cycles all shape what is appropriate. When those perspectives are aligned early, specifications become clearer and procurement becomes less reactive.
Table 1: Major Equipment Covered by the Specifications
Table 1 is the fastest way to align stakeholders: “radiotherapy equipment” is not just a treatment unit. It is a connected set of devices and software that enables planning, delivery, recording, verification, QA, and radiation protection.
| Category | Items |
|---|---|
| Major treatment equipment |
|
| Associated imaging equipment |
|
| Planning software |
|
| Information management software |
|
| Ancillary equipment |
|
Source: WHO/IAEA Technical Specifications of Radiotherapy Equipment for Cancer Treatment (Table 1).
Two practical notes help interpret this list. First, the document separates “ancillary clinical items” (trays, dressings, forceps, anaesthesia units, and so on) from the radiotherapy-technology scope because those are already covered elsewhere in priority-device lists. Second, within the scope, the information layer is treated as fundamental. When the publication lists TPS and OIS (including RVS), it is describing a service where planning, recording, and verification are not optional add-ons.
The executive summary also points out where the “real work” lives when you need to compare vendors or write a tender: the annexes contain detailed standard template technical specification tables for major equipment items. That matters because it pushes teams to be explicit about what is required (and why), and it keeps conversations anchored in standards, safety measures, and QA expectations rather than marketing language.
If you want to strengthen that interoperability perspective within the blog, two relevant internal reads are the practical DICOM guide for medical imaging systems and the article on DICOM networking (SOPs, DIMSE and AE configuration). They help connect the “DICOM-compatible” requirement in planning systems to what it means in real networks and integrations.
Chapter 2: EBRT, Brachytherapy, and Equipment Packages
Chapter 2 separates radiotherapy into EBRT and brachytherapy and then translates that split into equipment packages linked to health-system capacity, anchored by an explicit needs-assessment approach.
The definition is straightforward. In EBRT, the ionizing radiation source is external to the patient. In brachytherapy, the source is internal or in close proximity to the patient. The text also offers a useful global snapshot: the worldwide ratio of EBRT treatment units to brachytherapy treatment units is more than 9 to 1, based on the IAEA DIRAC database. That helps explain why standalone EBRT services are common and why brachytherapy is often referred out.
Even so, the publication’s working assumption is a radiotherapy service that provides both EBRT and brachytherapy. It calls that comprehensive model essential for cervical cancer, where a course of EBRT is typically concurrent with a course of brachytherapy.
Needs Assessment: What You Have vs. What You Should Have
The chapter’s method is pragmatic. Start from a standard of what should be available (priority-device lists and national cancer-control strategies can serve as references). Measure what is actually available at facility, regional, or national level. The gap between the current state and the standard defines the overall need. Then comes the part that cannot be skipped: review financial and human resources required to address that gap, and if resources are constrained, prioritize with input from those commissioning the service, service providers, and service users.
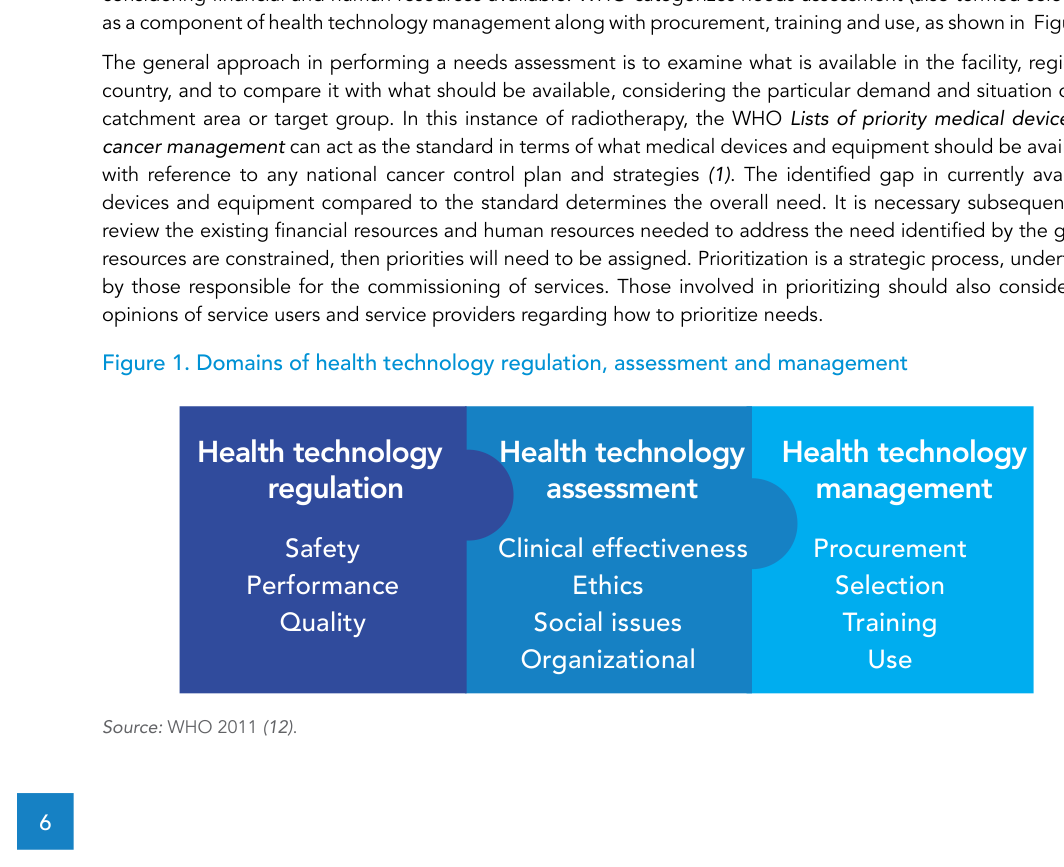
The chapter explicitly frames selection as one component of health technology management, alongside procurement, training, and use. That framing is more than semantics. It signals that radiotherapy decisions must be governed: regulation focuses on safety, performance, and quality; assessment focuses on clinical effectiveness, ethics, and organizational and social considerations; and management covers procurement, selection, training, and use as ongoing responsibilities.
| Regulation | Assessment | Management |
|---|---|---|
|
|
|
Source: WHO/IAEA Technical Specifications of Radiotherapy Equipment for Cancer Treatment (Figure 1; Source: WHO 2011).
Table 2: EBRT Equipment Packages
Table 2 lays out three progressive packages. The publication states that detailed technical specifications cover Packages 1 and 2 (appropriate in limited-resource settings and including necessary ancillary equipment), while the additional capabilities in Package 3 are not specified in detail in the current document, although they may be developed by well-established departments using the same framework.
| Component (EBRT) | Package 1 | Package 2 | Package 3 |
|---|---|---|---|
| Treatment unit | Cobalt-60 teletherapy unit (preferably at least one with 100 cm SAD) and/or single-photon energy LINAC; orthovoltage X-ray unit as needed | Package 1 plus additional single-photon energy unit(s) and/or multiple energy LINAC with electrons capabilities | Additional multiple energy LINACs with electrons and IMRT, VMAT, IGRT, SRS, SBRT capabilities |
| Treatment unit accessories | Laser system for positioning; standard and customized shielding blocks; OIS including record and verify system (OIS including RVS); portal imaging | Laser system for positioning; customized blocks with or without MLC; OIS including RVS; EPID | Laser system for positioning; MLC or mini-MLC or cones; OIS including RVS; EPID; in-room MV or kV imaging (for IGRT); motion management system (for IGRT); OIS including RVS |
| Treatment planning | 3D TPS (DICOM-compatible) | 3D TPS (DICOM-compatible) | 3D TPS with additional capabilities (IMRT, VMAT, IGRT, SRS, SBRT) |
| Simulation imaging | Conventional digital simulator with laser system; access to a CT scanner | Package 1 plus dedicated CT simulator with moveable laser system | CT simulator with moveable laser system and with additional 4DCT capability; access to MRI and/or PET/CT; fiducial markers |
Source: WHO/IAEA Technical Specifications of Radiotherapy Equipment for Cancer Treatment (Table 2).
Two subtleties deserve emphasis. First, the publication highlights options within a package, such as single-energy versus multiple-energy LINAC and the presence or absence of an MLC. The purpose of later technical sections is to support these decisions by describing advantages and disadvantages of options. Second, capacity planning is treated as a clinical risk issue, not just an operational convenience. When a new EBRT service is designed around a single treatment unit, a breakdown can stop treatments; a single-unit department may also struggle to meet future increases in demand. The document therefore points readers to the value of considering two external beam treatment units at an early planning stage and planning for expansion. For cobalt-60 teletherapy, it also notes the potential resource-sparing advantages of procuring one unit with 100 cm SAD and one with 80 cm SAD (with a reference to a specific section for detail).
One line in the chapter is easy to overlook but important when you are planning beyond “year one”: the publication notes that expanding a service from Package 1 to Package 2 to Package 3 should happen as resources permit, and that a fully resourced comprehensive service may include equipment across all three packages, adapted to local context. In other words, the packages are not labels for hospitals; they are a practical way to stage capability over time.
Recommended Deep Dive 1: Packages and Implementation
Chapter 2 gives you the conceptual bridge from “what should we buy?” to a structured needs assessment, prioritization, and technology-management pathway. In the dedicated follow-up, we go deeper into applying the equipment packages in planning and implementation, connecting identified gaps to workforce capacity and a realistic expansion strategy.
Recommended Deep Dive 2: EBRT Specifications (Chapter 3)
For EBRT, the publication describes a consistent item-level specification structure: a general description, relevant IEC and ISO standards, a detailed sample specification, measures for radiation safety and protection, and QA recommendations to support patient safety and treatment quality. To see how that structure is applied to EBRT equipment, read the detailed article on technical specifications for EBRT equipment.
Recommended Deep Dive 3: Accessories, Alignment, and Imaging (EBRT)
Lasers, shielding blocks, MLC, EPID, in-room imaging, and motion management are listed as package-dependent components that materially change service capability. For an item-by-item view of that ecosystem, see the dedicated article on treatment-unit accessories and associated systems.
Recommended Deep Dive 4: Dosimetry, Quality Control, and Radiation Safety
Even when conversations start with a treatment unit, the publication consistently treats QA and protection as part of the service package. Dosimetry and quality control equipment and radiation safety equipment are listed as core ancillary items, and QA recommendations are integral to the specification format. For that practical layer, read our detailed article on dosimetry and QC equipment and how they underpin patient safety.
Recommended Deep Dive 5: Superficial/Orthovoltage X-ray Units
The superficial/orthovoltage X-ray unit appears in the scope and is explicitly mentioned as “as needed” within Package 1. To understand where it fits and how it is handled in the specifications, see the dedicated article on superficial and orthovoltage units.
Recommended Deep Dive 6: Brachytherapy Specifications (Chapter 4)
Brachytherapy is framed as both distinct from EBRT and essential to a comprehensive service, particularly for cervical cancer. The afterloader is listed as a major treatment item, and the publication dedicates a chapter to brachytherapy equipment within the defined packages. For that deep dive, read the detailed article on technical specifications for brachytherapy equipment.
Chapter 5: Establishing a Comprehensive Radiotherapy Service
Chapter 5 shifts the focus from selecting devices to establishing a service: activities, personnel, and procurement as part of a broader implementation pathway.
In the executive summary, this chapter is described as an overview of how to establish a comprehensive radiotherapy service, including procurement of relevant medical devices. It encompasses a range of activities and related personnel and points to additional comprehensive publications. The value here is to keep commissioning teams focused on the whole system, not on isolated equipment purchases.
If you want that perspective translated into an operational workflow, see the dedicated article on service implementation, patient safety, and quality management, which links the publication’s logic to day-to-day planning and governance.
Chapter 6: Emerging Technologies and Health Technology Assessment
Chapter 6 is a reminder that radiotherapy technology keeps evolving. New devices and techniques emerge and should be assessed before deployment, particularly in limited-resource settings.
The chapter uses Health Technology Assessment (HTA) as the decision lens. The definition presented is broad: a systematic evaluation of the properties, effects, and impacts of health care technology, including direct intended consequences and indirect unintended consequences. Its purpose is to inform technology-related policy-making, and it is conducted by interdisciplinary groups using explicit analytical frameworks and a variety of methods.
In practical terms, the chapter describes HTA as including, but not limited to, cost–benefit analysis, review of evidence of efficacy and performance, review of the implementation process, and review of patient safety. The sections then highlight emerging technologies and techniques that warrant this kind of assessment for future deployment.
Electronic Brachytherapy
One example discussed is electronic brachytherapy, where sealed radioactive sources such as cobalt-60 and iridium-192 may be replaced by miniature X-ray tubes. The text notes promising early studies in cervical cancer applications. The potential advantages are operational and regulatory: avoiding regular source replacement and reducing the regulatory burden around safety and security of radioactive sources.
At the same time, the document is cautious. More studies are needed to confirm efficacy across treatment sites and to demonstrate reliability of miniature X-ray tubes. If tube replacement is required at short intervals, cost-effectiveness in limited-resource settings may become questionable. For decision-makers, that is the practical takeaway: lifecycle reliability and maintenance realities can make or break the value case.
Image-Guided and Adaptive Radiotherapy
The chapter also revisits imaging. Imaging has always been part of radiotherapy, but over the last 10–15 years, digital imaging and computer control have enabled more options in simulation and at the time of treatment. The text cites dedicated imaging for planning, such as MRI for cervix and prostate and PET-CT for lung and head-and-neck cancers, to improve target delineation.
In-room imaging at the time of treatment is framed as both a coverage tool and an added safety measure to ensure correct treatment position. When imaging is rapid and performed immediately before treatment, adaptive radiotherapy becomes possible: the plan can be modified based on “images of the day.” The chapter notes that many imaging options are listed in a table and reinforces that any additional imaging in simulation or guidance should be investigated through the HTA lens.
Final Notes
If you are building or upgrading a radiotherapy service, the publication’s most valuable contribution is how it structures the problem: clear scope, an explicit list of core items, progressive packages, and a needs-assessment method tied to regulation, assessment, and management.
Use this guide as your map. When you want to go deeper, follow the dedicated articles linked throughout the text; they were designed to move from “what belongs in the package” to “how to specify, procure, implement, and sustain quality.”
Credits and Reference
Based on Technical specifications of radiotherapy equipment for cancer treatment (2021), distributed under the Creative Commons CC BY-NC-SA 3.0 IGO licence, with ISBN 978-92-4-001998-0 (electronic version) and 978-92-4-001999-7 (print version). Figures and tables reproduced here are attributed to the original source.