Cloud teleradiology aims to unify distributed reading
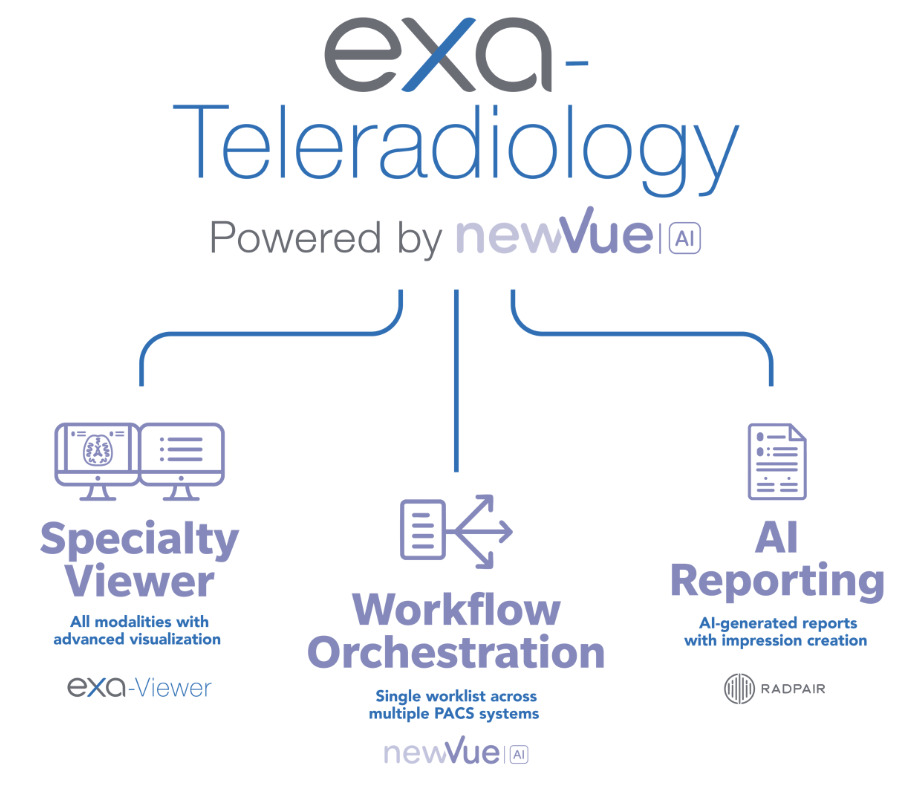
Cloud-based, browser-driven teleradiology platforms promise to solve a very concrete daily problem: bringing studies that today live scattered across multiple PACS and multiple facilities into a single reading environment. Instead of opening a separate workstation for every contract, hospital and viewer, the pitch is to concentrate workflow orchestration, a specialty viewer, AI-assisted reporting and imaging lifecycle management in one interface, billed per study. Konica Minolta Healthcare’s Exa Teleradiology is one recent example of the category, but the shift is industry-wide and worth understanding on its merits.
The forces behind this are familiar. Imaging demand is growing faster than the pipeline of new specialists, and those specialists are unevenly distributed across regions. As we have discussed, the radiologist shortage is a regional problem, not merely a headcount one: openings pile up outside the major hubs while supply concentrates in big cities. Remote, distributed reading has therefore become a structural answer rather than a convenience.
The “swivel-chair” problem: many worklists, many PACS
Anyone who covers several hospitals knows the phenomenon vendors have nicknamed “swivel-chair” reading: the radiologist spends the day jumping between workstations, worklists, logins and viewers, physically swiveling across monitors to serve different contracts. Every switch levies a cognitive tax — relearning shortcuts, reconfiguring windows, reconciling priorities — and every isolated login is one more chance for delay and error.
The promise of cloud workflow orchestration is to eliminate that back-and-forth. A unified worklist aggregates studies from different sources, applies routing rules (by subspecialty, urgency, contract or reader competency) and serves the most appropriate next case without the reader leaving the environment. In practice this moves teleradiology toward an “intelligent queue” model, where load distribution no longer depends on which PACS happens to be open.
Zero-footprint viewers and the end of the dedicated station
The zero-footprint viewer is the technical piece that makes this feasible. Unlike the old heavy clients that required installation, drivers and specific hardware, a zero-footprint viewer runs entirely in the browser: nothing is installed or left behind on the local machine. That lets radiologists read from almost any computer over a secure connection, simplifies IT maintenance and shrinks the attack surface — there is no outdated application accumulating vulnerabilities across dozens of desktops.
There are honest trade-offs. A diagnostic viewer in the browser depends on stable bandwidth, faithful rendering and calibrated monitors for primary interpretation; image fidelity and latency must be validated before it replaces a traditional diagnostic workstation. This cloud migration is part of the same digital transformation that reshaped PACS and imaging workflows over the past decade, and it demands the same commissioning rigor.
Generative-AI reporting: promise and caution
The newest layer in these platforms is generative-AI diagnostic reporting. The idea is to speed drafting — generating structured drafts, populating recurring findings, standardizing language and transcribing dictation — so the radiologist edits rather than types from scratch. Well tuned, this assistance can cut turnaround time and fatigue, especially on high-volume shifts.
Caution should scale with the enthusiasm. Generative models can hallucinate findings, propagate bias and produce plausible-but-wrong text. The radiologist remains accountable for the final report, and every AI draft must be treated as an auditable starting point, never as ground truth. Traceability of who reviewed and signed a report is a compliance requirement, not just a quality nicety.
Per-study pricing and the economics of cross-site reading
The “single price per study” model changes the operational math. Instead of perpetual licenses, on-premise servers and separate maintenance contracts for each component, a practice pays according to the volume it actually reads. For networks growing by acquisition, that lowers upfront investment and turns fixed cost into variable cost — attractive for seasonal or expanding operations.
But “per study” demands governance: without watching the exam mix and productivity, variable cost can escalate quickly during demand spikes. It is worth comparing against the scale gains already seen in the market — the growth of teleradiology built on modern PACS shows that volume and efficiency move together when the workflow is well designed. Imaging lifecycle management — storage tiers, retention and disposal — belongs in the same calculation and must be planned from day one.
Data sovereignty and compliance for cross-border cloud
For clinics operating internationally, or in Brazil specifically, cloud teleradiology raises an unavoidable question: where health data resides and under which laws. Regulations such as Brazil’s LGPD and Europe’s GDPR treat medical images and reports as sensitive personal data, requiring a legal basis, data minimization, processing records and well-defined processor contracts with the cloud provider. Server location, encryption in transit and at rest, and the possibility of cross-border transfers must be assessed before signing.
Data sovereignty is not a legal footnote: it defines who can access the images, in which jurisdiction a dispute would be heard, and how a security incident is handled. Institutions that have already been attacked know that cloud architectures concentrate value and, therefore, adversary attention. Choosing a vendor means auditing certifications, continuity plans and portability clauses so you are not locked into a single environment.
Practical implications and outlook
For radiologists and managers, the practical message is twofold. On one hand, cloud and browser platforms cut friction, unify worklists and can extend the reach of lean teams — exactly what regional scarcity demands. On the other, they require diagnostic validation of viewers, governance of AI reporting and disciplined data-protection compliance. Technology does not replace clinical judgment; it redistributes where that judgment is applied.
The multi-year trend points to consolidation: fewer isolated stations, more central orchestration, AI increasingly woven into the act of reporting, and elastic billing models. Offerings like Exa Teleradiology signal the direction, but any adoption decision should come from a measured pilot — turnaround time, quality, cost per study and security — not from marketing. Mature teleradiology will be the kind that unifies the workflow without diluting accountability.
Source: DOTmed — Exa Teleradiology by Konica Minolta Healthcare